Hypertension (HTN) – Complete Clinical Reference
1. Definition
Hypertension is a chronic condition characterized by persistently elevated systemic arterial blood pressure (BP), increasing the risk of cardiovascular, cerebrovascular, renal, and retinal disease.
- Office BP diagnosis:
≥140/90 mmHg on at least 2 separate visits
- Ambulatory/Home BP equivalents:
* Daytime ABPM ≥135/85 mmHg
* Night-time ABPM ≥120/70 mmHg
* 24-hour ABPM ≥130/80 mmHg
Reference:
https://www.escardio.org/Guidelines
https://www.heart.org/en/health-topics/high-blood-pressure
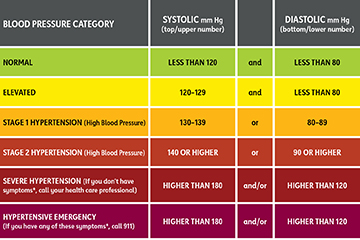
2. Classification (Adults)
| Category | Systolic (mmHg) | Diastolic (mmHg) |
| ------------------- | --------------- | ---------------- |
| Normal | <120 | <80 |
| Elevated | 120–129 | <80 |
| Stage 1 HTN | 130–139 | 80–89 |
| Stage 2 HTN | ≥140 | ≥90 |
| Hypertensive Crisis | ≥180 | ≥120 |
3. Epidemiology
- Affects >1.3 billion people worldwide
- Major modifiable risk factor for:
* Ischemic heart disease
* Stroke
* Chronic kidney disease
- Only ~50% of patients have adequate BP control
Reference:
https://www.who.int/news-room/fact-sheets/detail/hypertension
4. Etiology
A. Primary (Essential) Hypertension – ~90–95%
Multifactorial:
- Genetic predisposition
- High salt intake
- Obesity
- Sedentary lifestyle
- Insulin resistance
- Sympathetic overactivity
B. Secondary Hypertension – ~5–10%
| Cause | Key Clues |
| ------------------------- | ------------------------------------- |
| Renal parenchymal disease | Raised creatinine, abnormal urine |
| Renal artery stenosis | Abdominal bruit, ACEI creatinine rise |
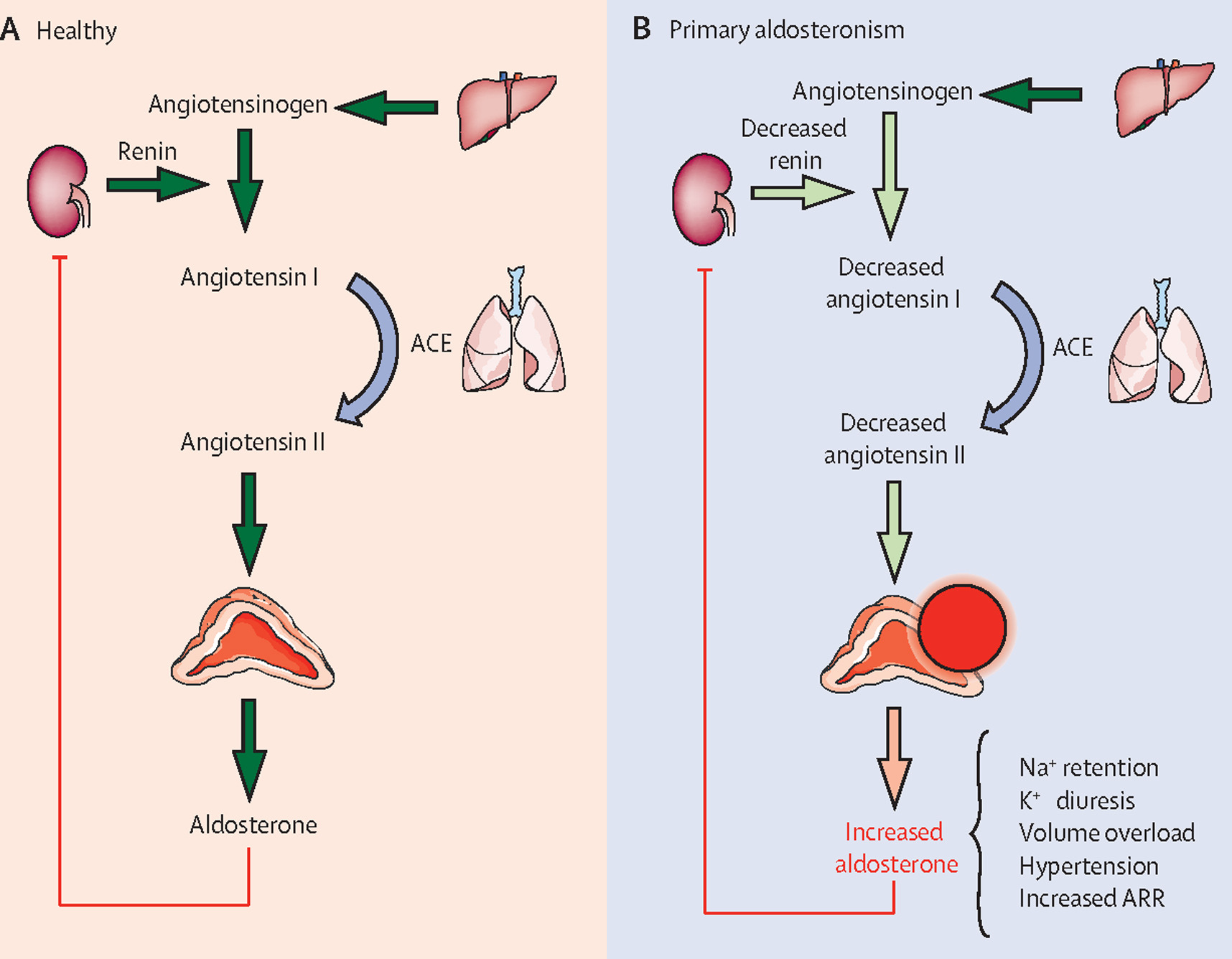
| Primary aldosteronism | Hypokalemia |
| Pheochromocytoma | Episodic headache, sweating |
| Cushing syndrome | Moon face, striae |
| OSA | Snoring, daytime sleepiness |
| Coarctation of aorta | BP arm > leg |
Reference:
https://www.uptodate.com/contents/secondary-hypertension
5. Pathophysiology
- Increased systemic vascular resistance
- Endothelial dysfunction
- RAAS activation → sodium retention
- Sympathetic nervous system overactivity
- Vascular remodeling → arterial stiffness
Leads to:
- Left ventricular hypertrophy
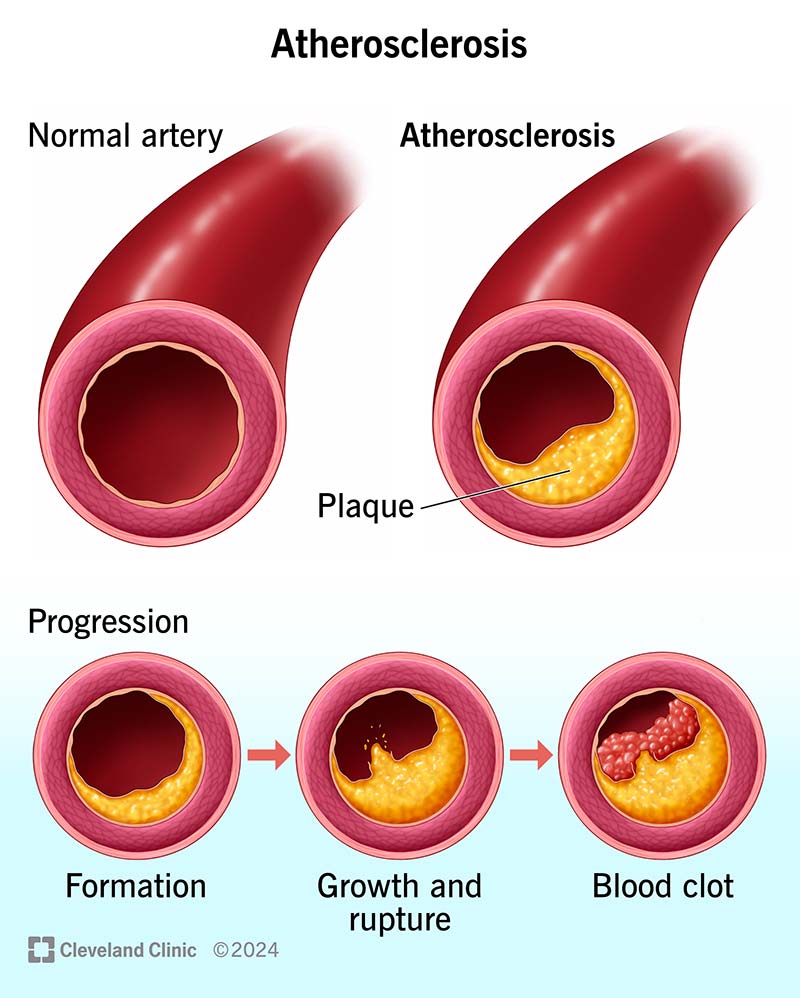
- Atherosclerosis
- Microvascular damage
6. Clinical Features
Usually Asymptomatic (“Silent Killer”)
Symptoms (when present)
- Headache
- Dizziness
- Blurred vision
- Chest pain
- Dyspnea
- Palpitations
Signs of Target Organ Damage
- LV hypertrophy
- Retinopathy
- Proteinuria
- Stroke/TIA
- Heart failure
7. Investigations
Baseline Evaluation
- BP (both arms)
- ECG
- Urinalysis
- Serum creatinine, eGFR
- Serum electrolytes
- Fasting glucose / HbA1c
- Lipid profile
Additional Tests (if indicated)
- Echocardiography (LVH)
- Renal Doppler / CT angiography
- Aldosterone–renin ratio
- Plasma metanephrines
- Sleep study (OSA)
Reference:
https://www.nice.org.uk/guidance/ng136
8. Differential Diagnosis
- White coat hypertension
- Masked hypertension
- Secondary hypertension
- Pseudohypertension (elderly)
- Anxiety-related BP elevation
9. Management (Stepwise)
A. Non-Pharmacological (For ALL patients)
| Measure | Expected BP Reduction |
| --------------------------- | --------------------- |
| Weight loss | ↓ 5–20 mmHg |
| Salt restriction (<5 g/day) | ↓ 5–6 mmHg |
| DASH diet | ↓ 8–14 mmHg |
| Exercise | ↓ 4–9 mmHg |
| Alcohol reduction | ↓ 2–4 mmHg |
Reference:
https://www.heart.org/en/healthy-living
B. Pharmacological Therapy
First-Line Drug Classes
- ACE inhibitors (ACEI)
- Angiotensin receptor blockers (ARB)
- Calcium channel blockers (CCB)
- Thiazide / thiazide-like diuretics
1. ACE Inhibitors (e.g., Enalapril)
- Indications: Diabetes, CKD, heart failure
- Mechanism: Inhibits angiotensin II formation
- Dose:
Adults: 5–40 mg/day
- Adverse effects: Cough, hyperkalemia, angioedema
- Contraindications: Pregnancy, bilateral renal artery stenosis
- Monitoring: Creatinine, potassium
- Counseling: Dry cough may occur
2. ARBs (e.g., Losartan)
- Indications: ACEI intolerance
- Mechanism: Blocks AT1 receptor
- Dose: 50–100 mg/day
- Adverse effects: Hyperkalemia
- Contraindications: Pregnancy
- Monitoring: Renal function
3. Calcium Channel Blockers (Amlodipine)
- Indications: Elderly, isolated systolic HTN
- Mechanism: Vasodilation via calcium blockade
- Dose: 5–10 mg/day
- Adverse effects: Pedal edema, flushing
- Contraindications: Severe aortic stenosis
4. Thiazide Diuretics (Chlorthalidone)
- Mechanism: Sodium excretion
- Dose: 12.5–25 mg/day
- Adverse effects: Hypokalemia, hyperuricemia
- Monitoring: Electrolytes
5. Beta Blockers (Selected Use)
- Indications: CAD, AF, heart failure
- Avoid: Asthma, severe bradycardia
10. Hypertensive Crisis
Hypertensive Emergency
- Severe BP + acute target organ damage
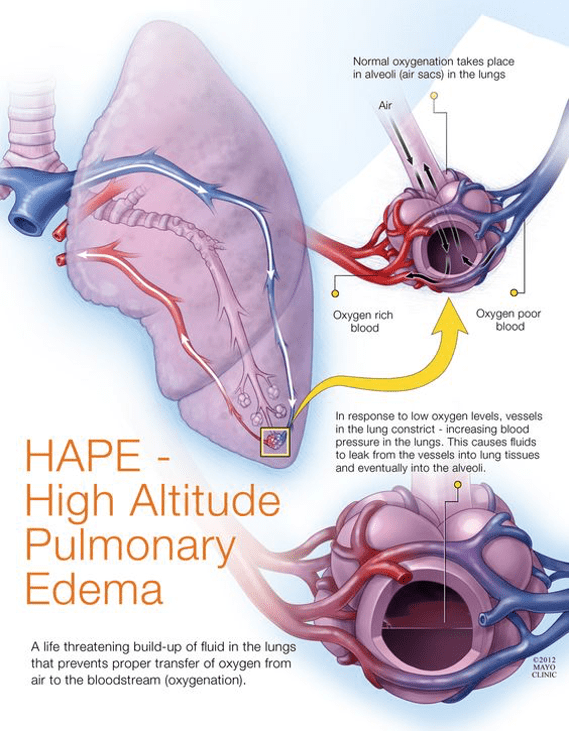
- Examples: Stroke, pulmonary edema, aortic dissection
Management
- ICU
- IV drugs (nitroprusside, labetalol, nitroglycerin)
- Reduce MAP by 20–25% in first hour
Hypertensive Urgency
- Severe BP without organ damage
- Oral drugs, gradual reduction
Reference:
https://www.acc.org/latest-in-cardiology
11. Special Situations
| Condition | Preferred Drugs |
| ----------------- | --------------------- |
| Pregnancy | Labetalol, Methyldopa |
| CKD + Proteinuria | ACEI / ARB |
| Diabetes | ACEI / ARB |
| Elderly | CCB, thiazide |
| BPH | Alpha blockers |
12. Complications
- Stroke
- Myocardial infarction
- Heart failure
- Chronic kidney disease
- Hypertensive retinopathy
- Aortic dissection
13. Target BP Goals
| Population | Target BP |
| -------------- | ------------ |
| General | <140/90 mmHg |
| Diabetes / CKD | <130/80 mmHg |
| Elderly (>65) | SBP 130–139 |
14. Patient Counseling Points
- Adherence is lifelong
- Home BP monitoring
- Avoid NSAIDs
- Lifestyle changes are mandatory
- Do not stop drugs abruptly
15. Key Authoritative External Resources
- WHO: https://www.who.int
- ESC Guidelines: https://www.escardio.org
- AHA: https://www.heart.org
- NICE: https://www.nice.org.uk
- UpToDate: https://www.uptodate.com