ADDISON’S DISEASE – COMPLETE CLINICAL REFERENCE
1. Definition
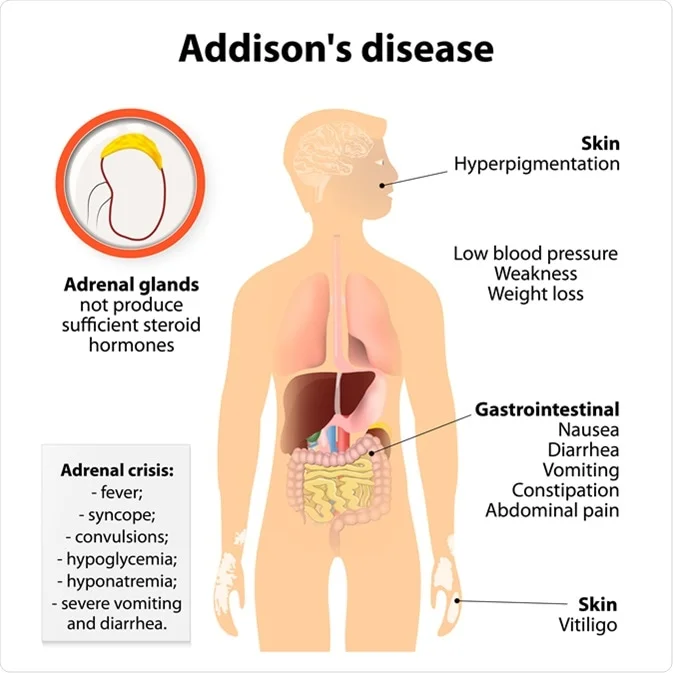
Addison’s disease is primary adrenal insufficiency, characterized by destruction or dysfunction of the adrenal cortex, leading to deficiency of cortisol, aldosterone, and adrenal androgens.
> It is a life-threatening endocrine disorder if untreated.
2. Pathophysiology
Loss of adrenal cortex function causes:
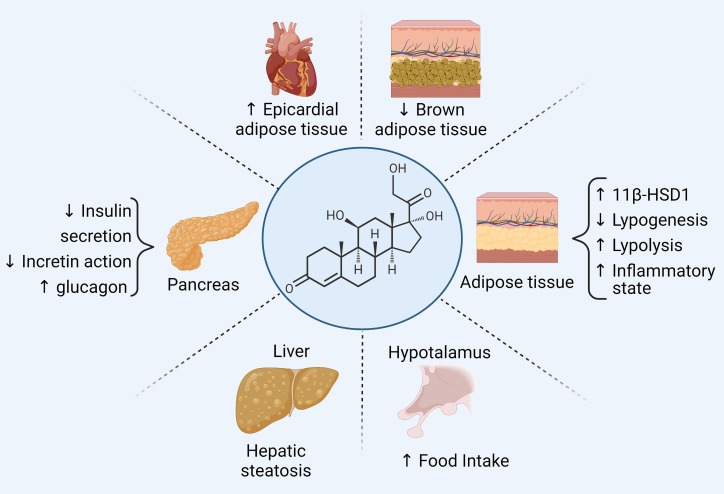
Cortisol Deficiency
- ↓ Gluconeogenesis → hypoglycemia
- ↓ Vascular responsiveness → hypotension
- ↓ Stress response → adrenal crisis
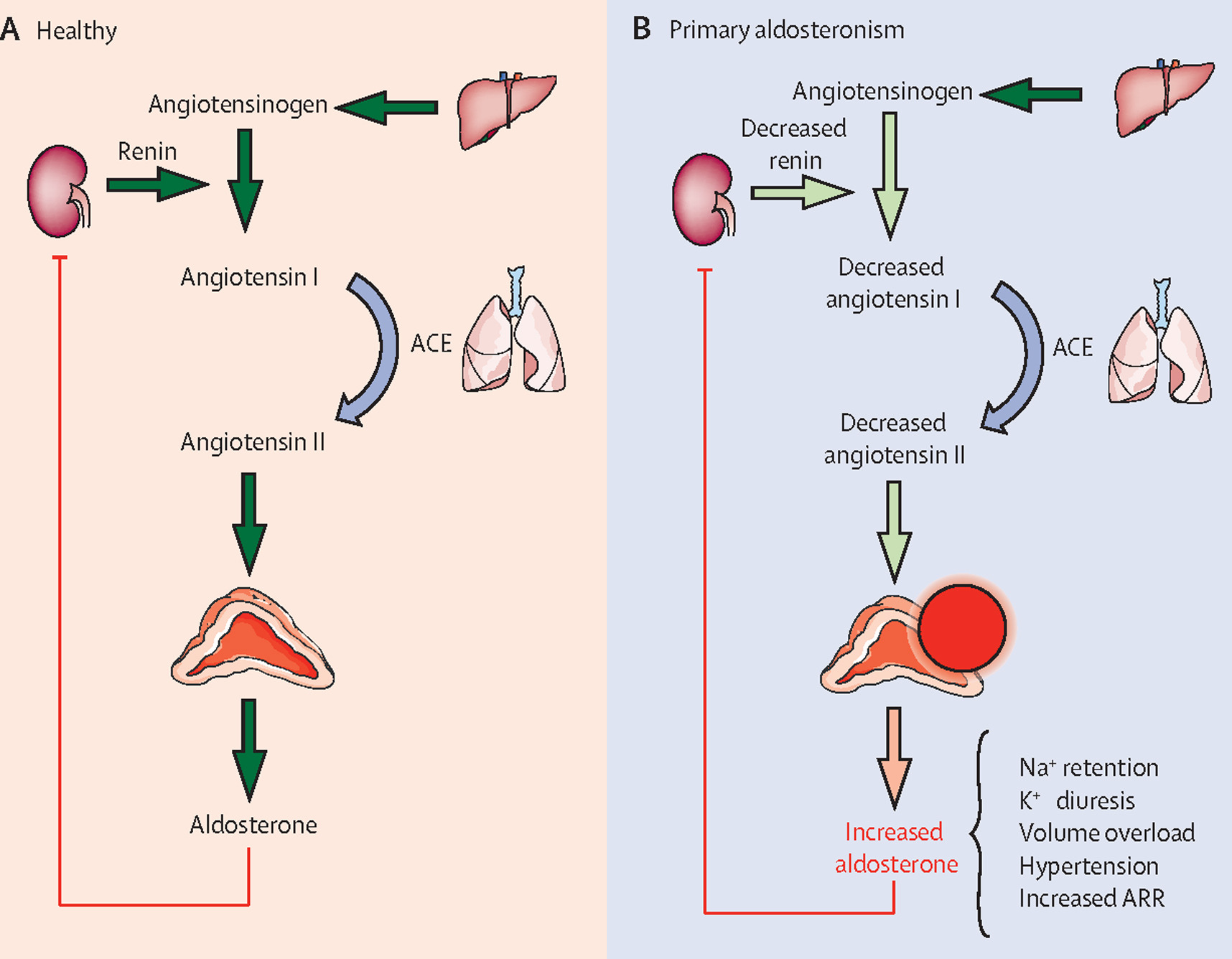
Aldosterone Deficiency
- ↓ Sodium reabsorption → hyponatremia
- ↓ Potassium excretion → hyperkalemia
- ↓ Intravascular volume → shock
ACTH Excess (Loss of negative feedback)
- ↑ ACTH → hyperpigmentation
- ↑ POMC → ↑ MSH
3. Etiology / Causes
A. Autoimmune (Most Common in Developed Countries)
- Autoimmune adrenalitis
- Associated with:
* Hashimoto thyroiditis
* Type 1 diabetes
* Pernicious anemia
* Vitiligo
(Autoimmune polyglandular syndrome type 2)
B. Infections
- Tuberculosis (most common worldwide)
- HIV
- Fungal infections (Histoplasma)
C. Infiltrative / Destructive
- Metastasis (lung, breast)
- Amyloidosis
- Sarcoidosis
- Hemochromatosis
D. Genetic
- Congenital adrenal hyperplasia
- Adrenoleukodystrophy
E. Drug-Induced
- Ketoconazole
- Etomidate
- Immune checkpoint inhibitors
4. Clinical Features
General
- Chronic fatigue
- Weight loss
- Anorexia
- Weakness
Skin & Mucosa
- Hyperpigmentation (palmar creases, knuckles, buccal mucosa)
- Vitiligo (autoimmune)
Cardiovascular
- Postural hypotension
- Shock (in crisis)
Gastrointestinal
- Nausea
- Vomiting
- Abdominal pain
- Diarrhea
Metabolic / Electrolytes
- Hyponatremia
- Hyperkalemia
- Hypoglycemia
- Metabolic acidosis
Neuropsychiatric
- Depression
- Irritability
- Cognitive slowing
Reproductive
- Loss of axillary and pubic hair (women)
- Decreased libido
5. Investigations / Diagnosis
Step 1: Baseline Labs
- Low serum cortisol (morning)
- High ACTH
- Hyponatremia
- Hyperkalemia
- Hypoglycemia
Step 2: ACTH (Cosyntropin) Stimulation Test – Gold Standard
- Cortisol measured at 0 and 30–60 minutes
- Failure to rise >18–20 µg/dL confirms Addison’s disease
Step 3: Etiology Workup
- Anti-21 hydroxylase antibodies
- CT abdomen (TB, calcification, metastasis)
- HIV / TB testing
6. Differential Diagnosis
- Secondary adrenal insufficiency
- Tertiary adrenal insufficiency
- SIADH
- Chronic fatigue syndrome
- Hypothyroidism
7. Management (Stepwise)
A. Chronic Management (Lifelong)
1. Glucocorticoid Replacement
Hydrocortisone
- Indication: Cortisol replacement
- MOA: Replaces deficient cortisol
- Dose (Adult): 15–25 mg/day in divided doses
- Pharmacokinetics: Short acting
- Adverse effects: Weight gain, osteoporosis (overdose)
- Monitoring: BP, weight, symptoms
- Counselling: Never stop abruptly
2. Mineralocorticoid Replacement
Fludrocortisone
- Indication: Aldosterone deficiency
- Dose: 0.05–0.2 mg/day
- Adverse effects: Hypertension, hypokalemia
- Monitoring: BP, electrolytes
- Counselling: Increase salt intake
B. Stress Dose Adjustment
- Double or triple dose during illness
- IM hydrocortisone if vomiting
C. Addisonian Crisis (Medical Emergency)
Features
- Severe hypotension
- Shock
- Vomiting
- Hypoglycemia
- Hyperkalemia
Treatment
- IV hydrocortisone 100 mg bolus → 50 mg q6h
- IV normal saline + dextrose
- Correct electrolytes
- Treat precipitating cause
8. Complications
- Addisonian crisis
- Severe hypotension
- Electrolyte imbalance
- Death if untreated
9. Special Situations
Pregnancy
- Continue replacement
- Increase dose in labor
Surgery / Trauma
- Mandatory stress dosing
10. Prognosis
- Excellent with compliance
- Poor if undiagnosed or non-adherent
11. Key Exam Pearls
- Hyperpigmentation = primary adrenal failure
- Hyperkalemia excludes secondary adrenal insufficiency
- Most common cause worldwide: TB
- Gold standard: ACTH stimulation test
- Never stop steroids abruptly