Differential Diagnosis of Jaundice (Complete Detailed Guide)
Definition
Jaundice = yellow discoloration of skin, sclera, and mucous membranes due to elevated serum bilirubin (>2–3 mg/dL).
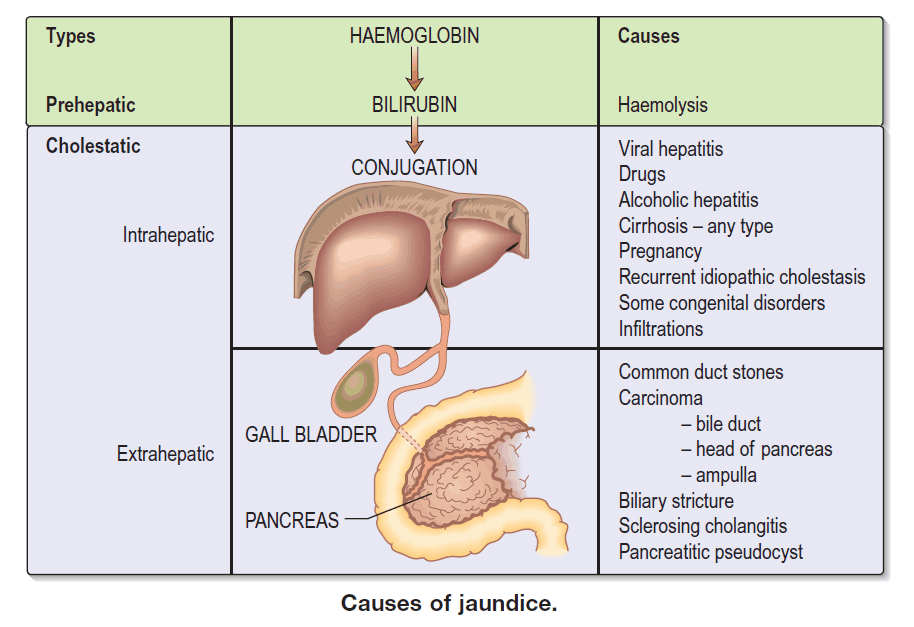
Physiological Classification
Jaundice is classified based on where bilirubin metabolism is impaired:
| Type | Mechanism | Bilirubin Type |
| ------------------------------ | --------------------------- | ---------------- |
| Pre-hepatic (Hemolytic) | Excess bilirubin production | Unconjugated |
| Hepatic (Hepatocellular) | Liver cell dysfunction | Mixed |
| Post-hepatic (Obstructive) | Impaired bile excretion | Conjugated |
1. Pre-Hepatic (Unconjugated) Jaundice
Cause: Increased bilirubin production due to hemolysis or ineffective erythropoiesis
Key Features
- No bilirubin in urine
- Normal or pale stool
- Elevated indirect bilirubin
- Increased reticulocyte count
Differential Diagnoses
Hemolytic Disorders
- Autoimmune hemolytic anemia
- Sickle cell disease
- Thalassemia
- G6PD deficiency
- Hereditary spherocytosis
- Malaria
- Transfusion reactions
Ineffective Erythropoiesis
- Megaloblastic anemia (B12/folate deficiency)
- Myelodysplastic syndrome
Other Causes
- Large hematoma resorption
- Neonatal physiologic jaundice
2. Hepatic (Hepatocellular) Jaundice
Cause: Liver cell injury impairing bilirubin uptake, conjugation, or secretion
Key Features
- Mixed conjugated + unconjugated bilirubin
- Elevated ALT/AST
- Dark urine may be present
- Variable stool color
A. Acute Hepatic Causes
Viral Hepatitis
- Hepatitis A, B, C, D, E
- Epstein–Barr virus (EBV)
- Cytomegalovirus (CMV)
Drug-Induced Liver Injury
- Acetaminophen (Paracetamol)
- Anti-tubercular drugs (INH, Rifampicin)
- Methotrexate
- Statins
- Herbal toxins
Alcoholic Hepatitis
Ischemic Hepatitis
- Shock liver
- Heart failure
Acute Liver Failure
- Viral, toxic, autoimmune causes
B. Chronic Hepatic Causes
Chronic Liver Disease
- Cirrhosis (alcoholic, viral, NAFLD)
- Chronic hepatitis B or C
- Autoimmune hepatitis
Metabolic Liver Diseases
- Wilson disease
- Hemochromatosis
- Alpha-1 antitrypsin deficiency
- Non-alcoholic fatty liver disease (NAFLD)
Infiltrative Diseases
- Hepatocellular carcinoma
- Liver metastases
- Lymphoma
- Amyloidosis
C. Genetic / Functional Hepatic Disorders
Unconjugated Hyperbilirubinemia
- Gilbert syndrome
- Crigler–Najjar syndrome
Conjugated Hyperbilirubinemia
- Dubin–Johnson syndrome
- Rotor syndrome
3. Post-Hepatic (Obstructive / Cholestatic) Jaundice
Cause: Obstruction of bile flow
Key Features
- Elevated conjugated bilirubin
- Dark urine
- Pale/clay-colored stool
- Pruritus
- Elevated ALP & GGT
A. Extrahepatic Obstruction
Gallstone Disease
- Choledocholithiasis
Malignancies
- Pancreatic cancer
- Cholangiocarcinoma
- Ampullary carcinoma
- Gallbladder cancer
Benign Strictures
- Post-surgical biliary stricture
- Primary sclerosing cholangitis (PSC)
External Compression
- Enlarged lymph nodes
- Pancreatic pseudocyst
B. Intrahepatic Cholestasis
Inflammatory / Autoimmune
- Primary biliary cholangitis (PBC)
- PSC
Drug-Induced Cholestasis
- Oral contraceptives
- Chlorpromazine
- Anabolic steroids
Sepsis-related cholestasis
Pregnancy-related
- Intrahepatic cholestasis of pregnancy
4. Neonatal Jaundice Differential
Physiologic
- Immature bilirubin conjugation
Pathologic
- ABO/Rh hemolytic disease
- Sepsis
- Biliary atresia
- Neonatal hepatitis
- Crigler–Najjar syndrome
- G6PD deficiency
5. Key Diagnostic Clues for Differentiation
| Feature | Pre-Hepatic | Hepatic | Post-Hepatic |
| ------------- | ----------- | ----------- | ------------- |
| Urine color | Normal | Dark | Dark |
| Stool color | Normal | Normal/pale | Pale/clay |
| ALT/AST | Normal | High | Mild |
| ALP/GGT | Normal | Mild | Very high |
| Reticulocytes | High | Normal | Normal |
| Pruritus | No | Sometimes | Severe |
6. Differential Based on Bilirubin Pattern
Predominantly Unconjugated
- Hemolysis
- Gilbert syndrome
- Crigler–Najjar
- Neonatal jaundice
Predominantly Conjugated
- Obstructive jaundice
- PSC / PBC
- Biliary malignancy
- Dubin–Johnson syndrome
Mixed
- Hepatitis
- Cirrhosis
- Alcoholic liver disease
- Drug-induced liver injury
7. Red-Flag Causes That Must Not Be Missed
- Acute liver failure
- Pancreatic cancer
- Cholangiocarcinoma
- Biliary atresia (infants)
- Sepsis-related jaundice
- Drug toxicity
8. Quick Clinical Pattern-Based Differential
Painless progressive jaundice
- Pancreatic cancer
- Cholangiocarcinoma
- Ampullary carcinoma
Painful jaundice with fever
- Acute cholangitis
- Gallstones
- Liver abscess
Jaundice with anemia
- Hemolytic anemia
- G6PD deficiency
- Thalassemia
Jaundice with weight loss
- Malignancy
- Chronic liver disease
Jaundice with pruritus
- Cholestasis
- PBC / PSC
9. Diagnostic Workup to Narrow Differential
Laboratory Tests
- Total, direct, indirect bilirubin
- ALT, AST, ALP, GGT
- CBC, reticulocyte count
- PT/INR, albumin
- Viral hepatitis markers
- Autoimmune markers
- Hemolysis profile (LDH, haptoglobin)
Imaging
- Ultrasound abdomen
- MRCP / ERCP if obstruction suspected
- CT scan if malignancy suspected
10. Summary Flow for Differential Approach
Step 1: Determine bilirubin type
Step 2: Assess liver enzymes pattern
Step 3: Evaluate urine & stool color
Step 4: Rule out hemolysis
Step 5: Look for obstruction
Step 6: Screen for liver disease & malignancy