Crohn’s Disease – Complete Reference
1. Definition
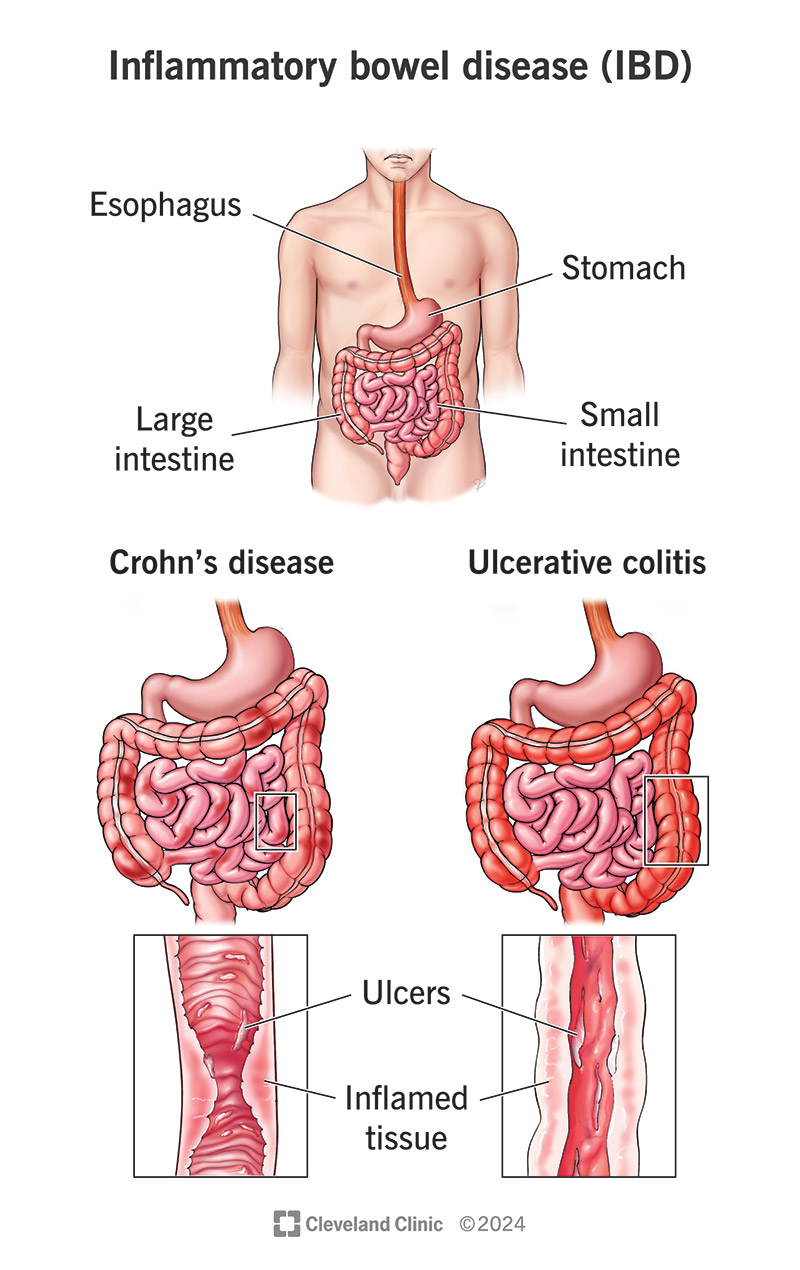
Crohn’s disease (CD) is a chronic, relapsing–remitting inflammatory bowel disease (IBD) characterized by transmural inflammation that can affect any part of the gastrointestinal tract from mouth to anus, most commonly the terminal ileum and colon, with skip lesions.
2. Epidemiology
- Peak onset: 15–35 years
- Second peak: 50–70 years
- Slight female predominance
- Higher prevalence in Western countries
- Increased risk with smoking
3. Etiopathogenesis (Pathophysiology)
A. Genetic Factors
- NOD2/CARD15 mutations → impaired bacterial recognition
- Other genes: ATG16L1, IL23R
- Stronger genetic link than ulcerative colitis
B. Immune Dysregulation
- Th1 and Th17–mediated immune response
- Excess cytokines:
* TNF-α
* IL-12
* IL-23
- Loss of immune tolerance to gut microbiota
C. Environmental Triggers
- Cigarette smoking (worsens disease)
- NSAIDs
- Altered gut microbiome
D. Pathological Hallmarks
- Transmural inflammation
- Non-caseating granulomas
- Cobblestone mucosa
- Fistulae, strictures, abscesses
4. Sites of Involvement
- Terminal ileum (most common)
- Colon
- Ileocolonic
- Perianal region
- Upper GI (esophagus, stomach, duodenum – less common)
5. Clinical Features
A. Intestinal Symptoms
- Chronic diarrhea (± blood)
- Abdominal pain (often right lower quadrant)
- Weight loss
- Fatigue
- Fever during flares
B. Complications
- Intestinal strictures → obstruction
- Fistulae (entero-enteric, entero-cutaneous, entero-vesical)
- Abscess formation
- Malabsorption (B12, bile salts)
- Short bowel syndrome (post-surgery)
C. Perianal Disease
- Fissures
- Fistulas
- Perianal abscesses
- Skin tags
D. Extra-Intestinal Manifestations
- Joints: peripheral arthritis, ankylosing spondylitis
- Skin: erythema nodosum, pyoderma gangrenosum
- Eyes: uveitis, episcleritis
- Hepatobiliary: primary sclerosing cholangitis (less common than UC)
- Renal: oxalate kidney stones
6. Investigations and Diagnosis
A. Laboratory Tests
- CBC → anemia
- ESR, CRP ↑
- Hypoalbuminemia
- Vitamin B12 deficiency
- Stool calprotectin ↑ (marker of intestinal inflammation)
B. Endoscopy (Gold Standard)
- Colonoscopy with ileoscopy
- Findings:
* Skip lesions
* Aphthous ulcers
* Cobblestone appearance
- Biopsy:
* Transmural inflammation
* Non-caseating granulomas (not always present)
C. Imaging
- MR enterography / CT enterography
* Fistulae
* Abscesses
* Strictures
- Barium studies:
* “String sign” (terminal ileum narrowing)
D. Differential Diagnosis
- Ulcerative colitis
- Intestinal tuberculosis
- IBS
- Ischemic colitis
- Colon cancer
- Behçet disease
7. Disease Classification (Montreal)
Age at diagnosis
- A1: <16 years
- A2: 17–40 years
- A3: >40 years
Location
- L1: Ileal
- L2: Colonic
- L3: Ileocolonic
- L4: Upper GI
Behavior
- B1: Non-stricturing, non-penetrating
- B2: Stricturing
- B3: Penetrating (fistulas)
8. Management (Stepwise)
Goals
- Induce remission
- Maintain remission
- Prevent complications
- Improve quality of life
9. Pharmacologic Treatment
A. Aminosalicylates (Limited Role)
Drug: Mesalamine
- Indication: Mild colonic disease (limited efficacy)
- MOA: Inhibits prostaglandin and leukotriene synthesis
- Dose: 2–4 g/day oral
- Adverse effects: Headache, nephrotoxicity
- Monitoring: Renal function
B. Corticosteroids (Induction Only)
Drug: Prednisolone / Budesonide
- Indication: Moderate–severe flares
- MOA: Suppress inflammatory cytokines
- Dose:
* Prednisolone: 40–60 mg/day
* Budesonide: 9 mg/day (ileocecal disease)
- Adverse effects: Osteoporosis, diabetes, infection, adrenal suppression
- Contraindication: Long-term maintenance
- Counselling: Do not stop abruptly
C. Immunomodulators
1. Azathioprine / 6-Mercaptopurine
- Indication: Steroid-dependent disease, maintenance
- MOA: Purine synthesis inhibition → ↓ lymphocytes
- Dose: 2–2.5 mg/kg/day
- Adverse effects: Myelosuppression, pancreatitis, lymphoma
- Monitoring: CBC, LFTs, TPMT activity
2. Methotrexate
- Indication: Refractory Crohn’s
- Dose: 15–25 mg weekly IM/SC
- Adverse effects: Hepatotoxicity, teratogenicity
- Contraindicated in pregnancy
D. Biologic Therapy
1. Anti-TNF Agents
- Infliximab
- Adalimumab
MOA: Neutralize TNF-α
Indication: Moderate–severe, fistulizing Crohn’s
Adverse effects: TB reactivation, infections, lymphoma
Screening: TB, hepatitis B before starting
2. Anti-Integrin
- Vedolizumab (gut-selective)
3. Anti-IL-12/23
- Ustekinumab
E. Antibiotics
- Metronidazole
- Ciprofloxacin
Indication: Perianal disease, abscesses
10. Surgical Management
- Not curative
- Indications:
* Obstruction
* Perforation
* Abscess
* Refractory disease
- Common procedures:
* Strictureplasty
* Segmental resection
- High recurrence after surgery
11. Non-Pharmacologic Management
- Smoking cessation (very important)
- Nutritional support
- Vitamin B12, iron, vitamin D supplementation
- Low-residue diet during flares
- Vaccinations (before immunosuppression)
12. Complications
- Intestinal obstruction
- Fistulae
- Malnutrition
- Colorectal cancer (in long-standing disease)
- Growth failure in children
13. Prognosis
- Chronic lifelong disease
- Relapsing–remitting course
- Early biologic therapy improves outcomes
- Smoking worsens prognosis
14. Key Differences from Ulcerative Colitis (Quick Recall)
| Feature | Crohn’s | Ulcerative Colitis |
| ------------ | ------------ | ------------------ |
| Distribution | Skip lesions | Continuous |
| Depth | Transmural | Mucosal |
| Ileum | Common | Rare |
| Fistula | Common | Absent |
| Surgery | Not curative | Curative |