Cerebellum Anatomy
Introduction
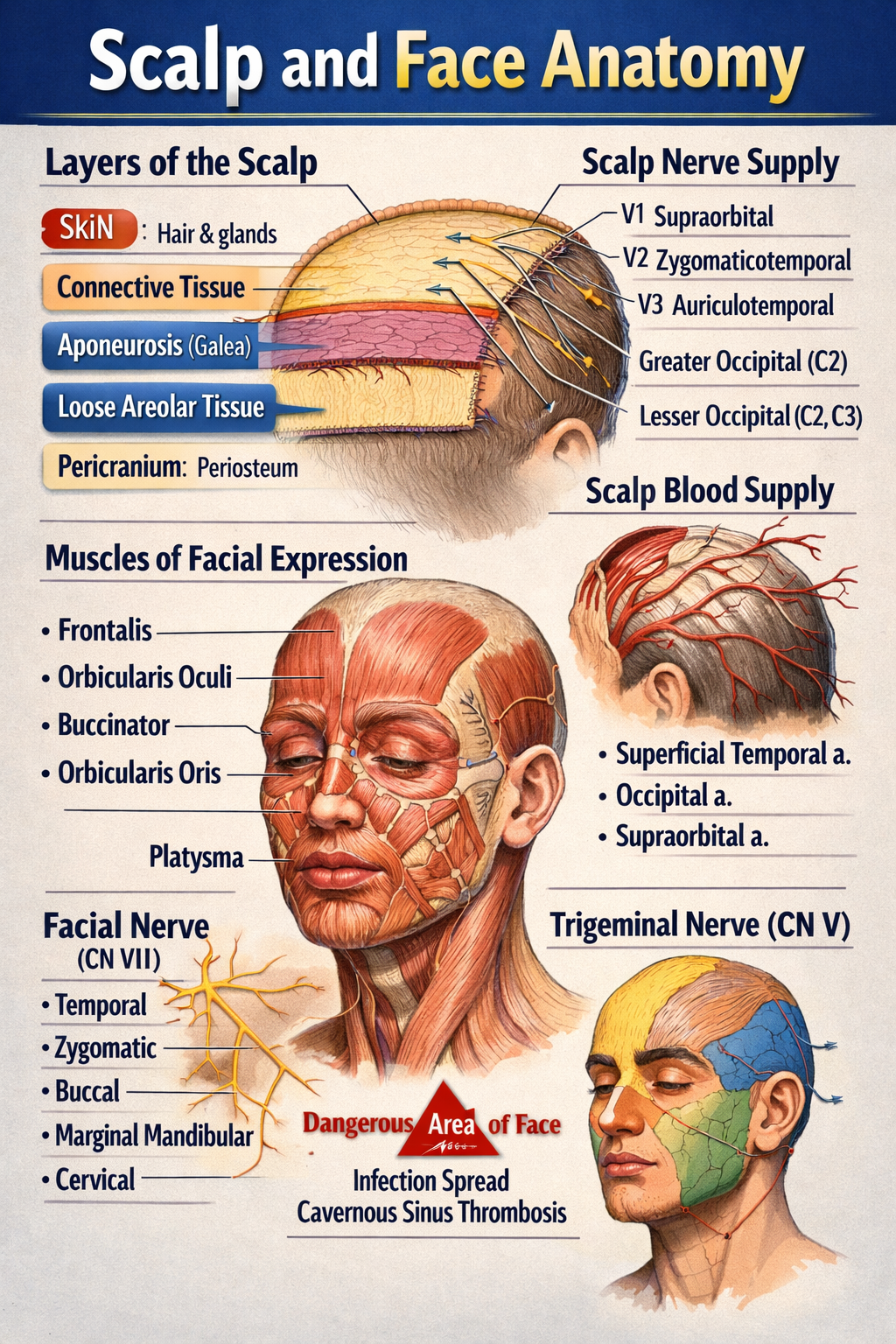
The cerebellum is a major part of the hindbrain that plays a critical role in coordination of movement, balance, posture, muscle tone, and motor learning. Although it does not initiate movement, it fine-tunes motor activity to ensure accuracy and smooth execution.
Location and Relations
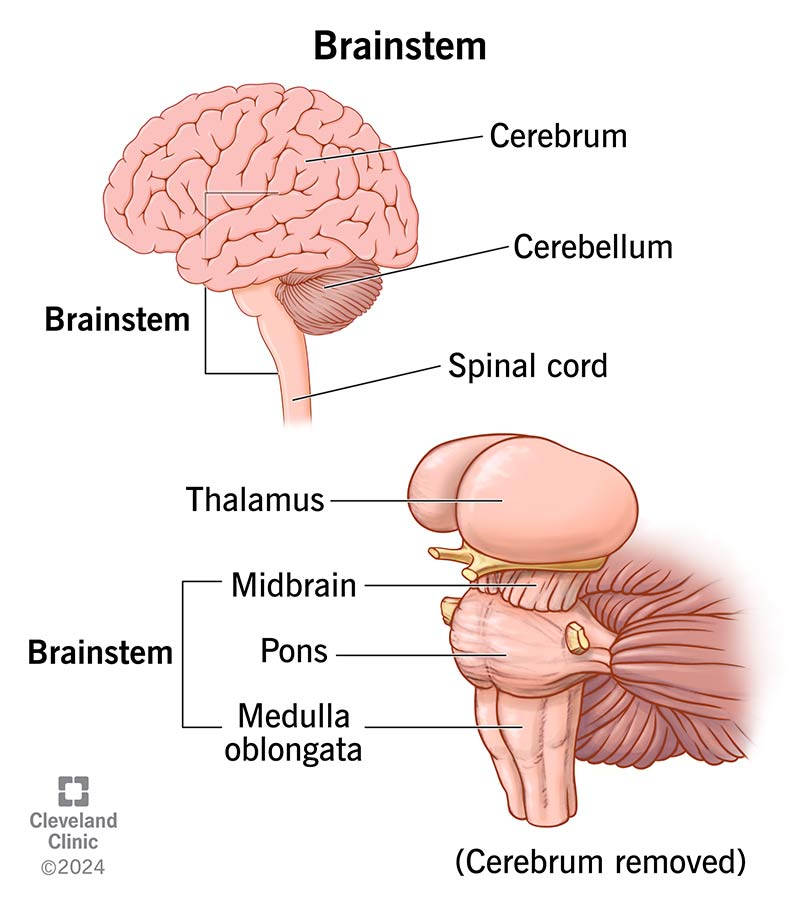
- Situated in the posterior cranial fossa
- Lies behind the pons and medulla
- Separated from the cerebrum by the tentorium cerebelli
- Forms the roof of the fourth ventricle
Gross Anatomy of the Cerebellum
External Features
The cerebellum consists of:
- Two hemispheres (right and left)
- Vermis (midline structure connecting hemispheres)
Surfaces
- Superior surface
- Inferior surface
- Both surfaces show numerous transverse folds called folia
Lobes of the Cerebellum
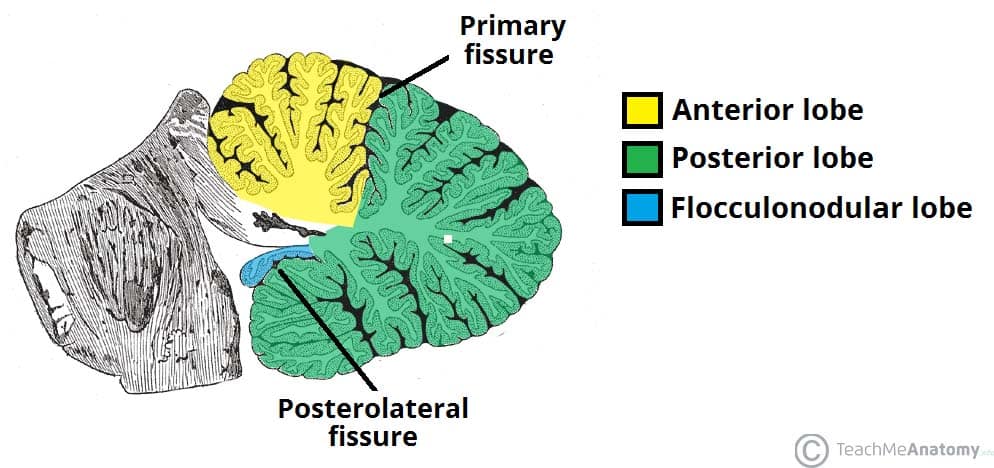
The cerebellum is divided by fissures into three lobes:
1. Anterior Lobe
- Located anterior to the primary fissure
- Functionally related to spinocerebellum
- Involved in posture and gait control
2. Posterior Lobe
- Largest lobe
- Lies between primary fissure and posterolateral fissure
- Involved in fine voluntary movements
3. Flocculonodular Lobe
- Composed of flocculus + nodulus
- Also called vestibulocerebellum
- Responsible for balance and eye movements
Functional Divisions of the Cerebellum
1. Cerebrocerebellum
- Lateral hemispheres
- Connected to cerebral cortex
- Controls planning and coordination of skilled movements
2. Spinocerebellum
- Vermis and intermediate zones
- Regulates muscle tone and ongoing movements
3. Vestibulocerebellum
- Flocculonodular lobe
- Maintains equilibrium and eye coordination
Cerebellar Cortex (Microscopic Anatomy)
Layers of Cerebellar Cortex
The cerebellar cortex has three layers:
- Molecular Layer
* Contains stellate and basket cells
* Few neurons, mostly fibers
- Purkinje Cell Layer
* Single layer of large Purkinje cells
* Output neurons of the cerebellar cortex
* Inhibitory (GABAergic)
- Granular Layer
* Contains granule cells and Golgi cells
* Highly cellular
White Matter of Cerebellum
- Located deep to the cortex
- Appears as arbor vitae (tree-like pattern)
- Carries fibers connecting cortex to cerebellar nuclei
Deep Cerebellar Nuclei
Embedded within white matter:
- Dentate
- Emboliform
- Globose
- Fastigial
These nuclei serve as major output centers of the cerebellum.
Cerebellar Peduncles
The cerebellum connects to the brainstem via three paired peduncles:
1. Superior Cerebellar Peduncle
- Connects to midbrain
- Mainly efferent (output) fibers
2. Middle Cerebellar Peduncle
- Connects to pons
- Largest peduncle
- Carries afferent fibers from cerebral cortex
3. Inferior Cerebellar Peduncle
- Connects to medulla
- Mixed afferent and efferent fibers
Blood Supply of the Cerebellum
- Superior cerebellar artery (SCA)
- Anterior inferior cerebellar artery (AICA)
- Posterior inferior cerebellar artery (PICA)
All arise from the vertebrobasilar system.
Functional Summary
- Coordinates voluntary movements
- Maintains posture and balance
- Regulates muscle tone
- Involved in motor learning and error correction
Clinical Correlation (Brief)
Lesions of the cerebellum lead to:
- Ataxia
- Dysmetria
- Intention tremor
- Nystagmus
- Hypotonia
- Scanning speech
SEO Title
Cerebellum Anatomy Structure Functions and Clinical Importance
Meta Description
Comprehensive SEO-friendly guide on cerebellum anatomy covering location lobes functional divisions cerebellar cortex peduncles blood supply and clinical significance.
SEO Keywords
cerebellum anatomy, cerebellar lobes, cerebellar cortex layers, cerebellar peduncles, deep cerebellar nuclei, cerebellum functions, hindbrain anatomy, neuroanatomy cerebellum
If you want next:
- 30 case-based cerebellar lesion scenarios
- Hard MCQs with explanations
- Clinical syndromes of cerebellar lesions
- HTML/CSS/JS exam-mode MCQs
Just tell me 👍
Below are high-yield clinical case scenarios of cerebellar lesions with clear diagnosis and management, written in an exam-oriented, clinical approach. Concise but complete.
1. Midline (Vermis) Lesion – Truncal Ataxia
Case
A 45-year-old man with chronic alcohol use presents with inability to sit or stand without support. Limb movements are relatively normal. Gait is broad-based and staggering.
Clinical Diagnosis
Vermian cerebellar lesion (anterior lobe degeneration)
Key Features
- Truncal ataxia
- Broad-based gait
- Minimal limb ataxia
Management
- Treat underlying cause (alcohol cessation)
- Thiamine supplementation
- Physiotherapy for gait and balance
- Fall-prevention measures
2. Cerebellar Hemisphere Lesion – Ipsilateral Limb Ataxia
Case
A 60-year-old man with hypertension presents with clumsiness of the right hand. Finger-nose test shows past pointing on the right.
Clinical Diagnosis
Right cerebellar hemisphere infarction
Key Features
- Ipsilateral limb ataxia
- Dysmetria
- Intention tremor
Management
- MRI brain to confirm stroke
- Antiplatelet therapy
- Blood pressure and risk factor control
- Neurorehabilitation
3. Flocculonodular Lobe Lesion – Balance Disorder
Case
A child presents with frequent falls, vertigo, and abnormal eye movements.
Clinical Diagnosis
Vestibulocerebellar lesion
Key Features
- Nystagmus
- Vertigo
- Severe balance impairment
Management
- Treat underlying cause (tumor/infection)
- Vestibular rehabilitation
- Anti-vertigo medications (short term)
4. Acute Cerebellar Stroke
Case
A 70-year-old patient presents with sudden onset vertigo, vomiting, ataxia, and headache.
Clinical Diagnosis
Cerebellar infarction (PICA/AICA territory)
Management
- Emergency CT/MRI brain
- Manage raised intracranial pressure
- Antiplatelet or anticoagulation as indicated
- Neurosurgical decompression if brainstem compression
5. Cerebellar Hemorrhage
Case
A hypertensive patient develops sudden headache, vomiting, and rapid deterioration of consciousness.
Clinical Diagnosis
Cerebellar hemorrhage
Management
- Immediate CT brain
- Blood pressure control
- Neurosurgical evacuation if large bleed
- ICU monitoring
6. Alcoholic Cerebellar Degeneration
Case
A chronic alcoholic presents with progressive gait instability over months.
Clinical Diagnosis
Anterior cerebellar lobe degeneration
Management
- Alcohol abstinence
- Nutritional rehabilitation
- Thiamine and multivitamins
- Long-term physiotherapy
7. Multiple Sclerosis with Cerebellar Involvement
Case
A young woman presents with intention tremor, scanning speech, and nystagmus.
Clinical Diagnosis
Cerebellar involvement in multiple sclerosis
Management
- MRI brain with contrast
- Acute relapse: corticosteroids
- Disease-modifying therapy
- Speech and occupational therapy
8. Cerebellar Tumor (Medulloblastoma)
Case
A child presents with morning vomiting, headache, and gait ataxia.
Clinical Diagnosis
Midline cerebellar tumor (medulloblastoma)
Management
- MRI brain
- Surgical excision
- Radiotherapy and chemotherapy
- Long-term neurodevelopmental follow-up
9. Cerebellar Abscess
Case
A patient with chronic otitis media presents with fever, headache, and ataxia.
Clinical Diagnosis
Cerebellar abscess
Management
- MRI with contrast
- IV broad-spectrum antibiotics
- Surgical drainage if indicated
- Treat source of infection
10. Drug-Induced Cerebellar Toxicity
Case
A patient on phenytoin presents with nystagmus and ataxia.
Clinical Diagnosis
Drug-induced cerebellar dysfunction
Management
- Check drug levels
- Stop or reduce offending drug
- Supportive care
- Monitor recovery
11. Paraneoplastic Cerebellar Degeneration
Case
A middle-aged woman presents with rapidly progressive ataxia; later found to have ovarian carcinoma.
Clinical Diagnosis
Paraneoplastic cerebellar degeneration
Management
- Treat underlying malignancy
- Immunotherapy (steroids, IVIG)
- Supportive rehabilitation
12. Cerebellar Ataxia in Hypothyroidism
Case
A patient presents with slow speech, unsteady gait, and fatigue.
Clinical Diagnosis
Metabolic cerebellar dysfunction
Management
- Thyroid function tests
- Thyroxine replacement
- Gradual neurological improvement
13. Arnold–Chiari Malformation
Case
A young adult presents with occipital headache worsened by coughing and gait imbalance.
Clinical Diagnosis
Chiari malformation affecting cerebellum
Management
- MRI brain and cervical spine
- Neurosurgical decompression if symptomatic
- Analgesia for headache
14. Post-Infectious Cerebellitis
Case
A child develops acute ataxia after viral illness.
Clinical Diagnosis
Acute cerebellitis
Management
- Usually self-limiting
- Supportive care
- Steroids if severe
- Physiotherapy
15. Degenerative Spinocerebellar Ataxia
Case
Progressive ataxia with positive family history.
Clinical Diagnosis
Spinocerebellar degeneration
Management
- Genetic testing
- Symptomatic treatment
- Rehabilitation
- Genetic counseling