Introduction
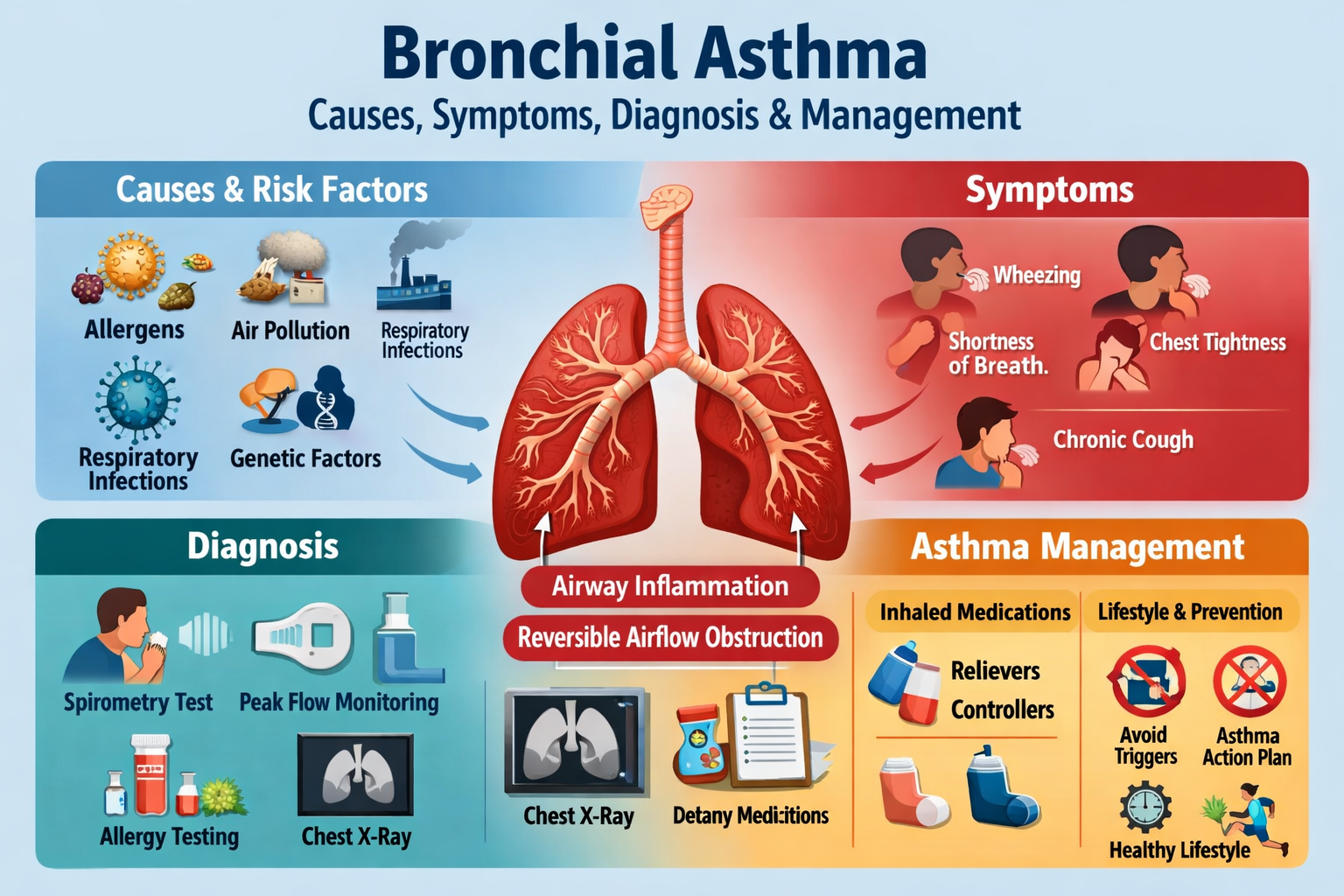
Bronchial asthma is a chronic inflammatory disease of the airways characterized by reversible airflow obstruction, bronchial hyper-responsiveness, and recurrent episodes of wheezing, breathlessness, chest tightness, and cough. It affects both children and adults and varies in severity from mild intermittent symptoms to life-threatening exacerbations.
Definition
Bronchial asthma is a chronic respiratory disorder in which exposure to specific triggers causes airway inflammation, smooth muscle constriction, and excessive mucus production, leading to airflow limitation that is usually reversible either spontaneously or with treatment.
Epidemiology
- Affects over 300 million people worldwide
- Common in children, but may persist or begin in adulthood
- Increasing prevalence in urban and industrialized areas
- Strong association with allergic diseases such as allergic rhinitis and eczema
Etiology and Risk Factors
Genetic Factors
- Family history of asthma or atopy
- Polymorphisms affecting immune regulation and airway responsiveness
Environmental Factors
- House dust mites
- Pollen
- Animal dander
- Mold spores
- Air pollution
- Tobacco smoke (active and passive)
Triggering Factors
- Respiratory viral infections
- Exercise (exercise-induced asthma)
- Cold air
- Emotional stress
- Occupational exposure (chemicals, flour, latex)
- Drugs (aspirin, NSAIDs, beta-blockers)
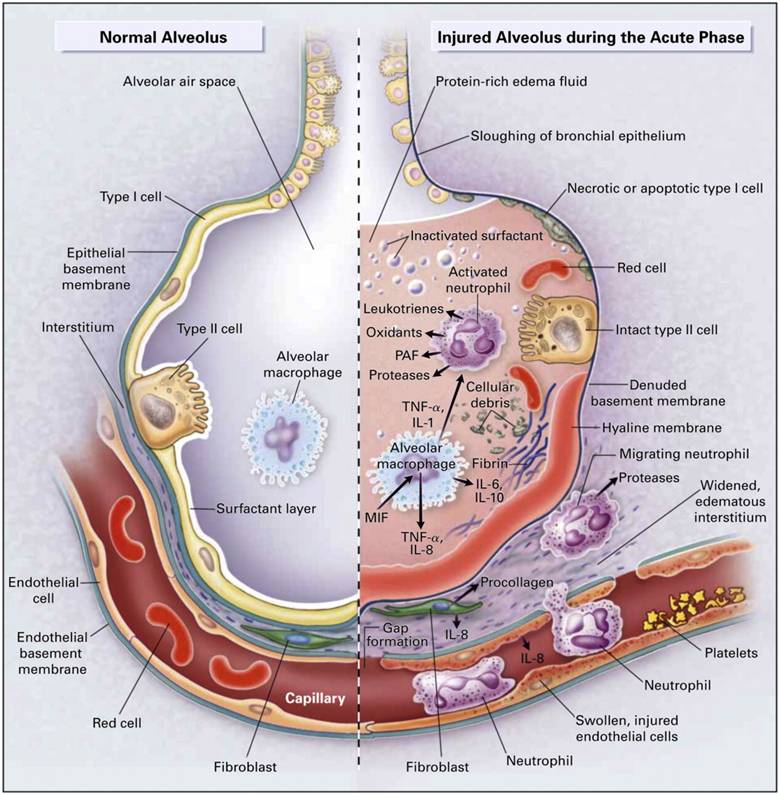
Pathophysiology
Asthma involves chronic airway inflammation with participation of:
- Eosinophils
- Mast cells
- T-helper 2 lymphocytes
Key mechanisms include:
- Bronchial smooth muscle contraction
- Airway edema
- Increased mucus secretion
- Airway remodeling in chronic disease
These changes cause narrowing of airways and airflow obstruction, leading to asthma symptoms.
Clinical Features
Typical Symptoms
- Episodic wheezing
- Shortness of breath
- Chest tightness
- Cough (often worse at night or early morning)
Signs on Examination
- Expiratory wheeze
- Prolonged expiration
- Use of accessory muscles in severe cases
- Reduced air entry during acute attacks
Classification of Asthma Severity
Based on Symptom Frequency
- Intermittent
- Mild persistent
- Moderate persistent
- Severe persistent
Based on Control Status
- Well-controlled
- Partly controlled
- Uncontrolled
Diagnosis
Clinical Diagnosis
- Recurrent respiratory symptoms with variable airflow limitation
- History of symptom variability and triggers
Pulmonary Function Tests
- Spirometry showing reduced FEV₁/FVC ratio
- Significant bronchodilator reversibility (FEV₁ improvement ≥12% and ≥200 mL)
Additional Investigations
- Peak expiratory flow monitoring
- Fractional exhaled nitric oxide (FeNO)
- Allergy testing (skin prick test or serum IgE)
- Chest X-ray (to exclude other conditions)
Differential Diagnosis
- Chronic obstructive pulmonary disease (COPD)
- Bronchiectasis
- Vocal cord dysfunction
- Cardiac asthma
- Pulmonary embolism
- Foreign body aspiration (especially in children)
Management of Bronchial Asthma
Goals of Treatment
- Symptom control
- Prevention of exacerbations
- Maintenance of normal lung function
- Minimal drug side effects
- Improved quality of life
Pharmacological Management
Reliever Medications
- Short-acting beta-2 agonists (SABA)
* Provide rapid bronchodilation
* Used for acute symptom relief
Controller Medications
- Inhaled corticosteroids (ICS) – cornerstone of therapy
- Long-acting beta-2 agonists (LABA) (always with ICS)
- Leukotriene receptor antagonists
- Long-acting muscarinic antagonists (LAMA)
- Biologic therapies (anti-IgE, anti-IL-5, anti-IL-4/13) for severe asthma
Stepwise Approach to Treatment
- Step 1: As-needed low-dose ICS with bronchodilator
- Step 2: Daily low-dose ICS
- Step 3: Low-dose ICS + LABA
- Step 4: Medium/high-dose ICS + LABA
- Step 5: Add biologics or oral corticosteroids
Management of Acute Asthma Exacerbation
- Oxygen therapy
- Frequent inhaled short-acting beta-2 agonists
- Systemic corticosteroids
- Anticholinergics in severe attacks
- Mechanical ventilation in life-threatening cases
Non-Pharmacological Management
- Avoidance of known triggers
- Smoking cessation
- Vaccination (influenza, pneumococcal)
- Patient education and inhaler technique training
- Written asthma action plan
- Weight management and regular physical activity
Complications
- Status asthmaticus
- Respiratory failure
- Recurrent hospitalizations
- Airway remodeling with fixed airflow limitation
- Reduced quality of life
Prevention and Prognosis
- Early diagnosis and proper treatment improve long-term outcomes
- Most patients achieve good control with appropriate therapy
- Poor adherence and continued exposure to triggers worsen prognosis
Conclusion
Bronchial asthma is a chronic but controllable respiratory disease. With early diagnosis, trigger avoidance, regular inhaled therapy, and patient education, most individuals can lead a normal, active life with minimal symptoms and reduced risk of severe exacerbations.