**Basic Life Support (BLS)
1. Definition
Basic Life Support (BLS) is the immediate, lifesaving care provided to a person with cardiac arrest, respiratory arrest, or airway obstruction until advanced medical care becomes available.
It focuses on early recognition, high-quality CPR, rapid defibrillation, and effective ventilation.
2. Objectives of BLS
- Maintain airway patency
- Support breathing and oxygenation
- Maintain circulation and perfusion of vital organs
- Prevent irreversible brain injury
- Increase survival and neurological outcomes
3. BLS Chain of Survival
- Early recognition and activation of emergency response
- Early high-quality CPR
- Early defibrillation (AED)
- Advanced life support
- Post–cardiac arrest care
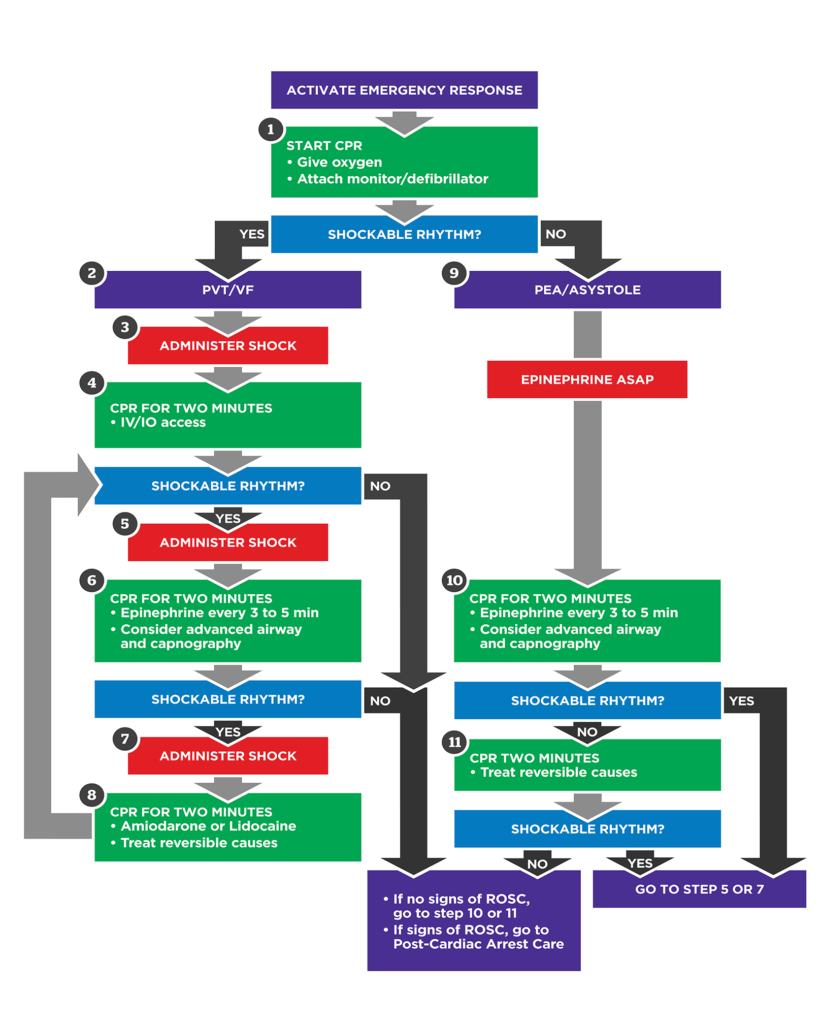
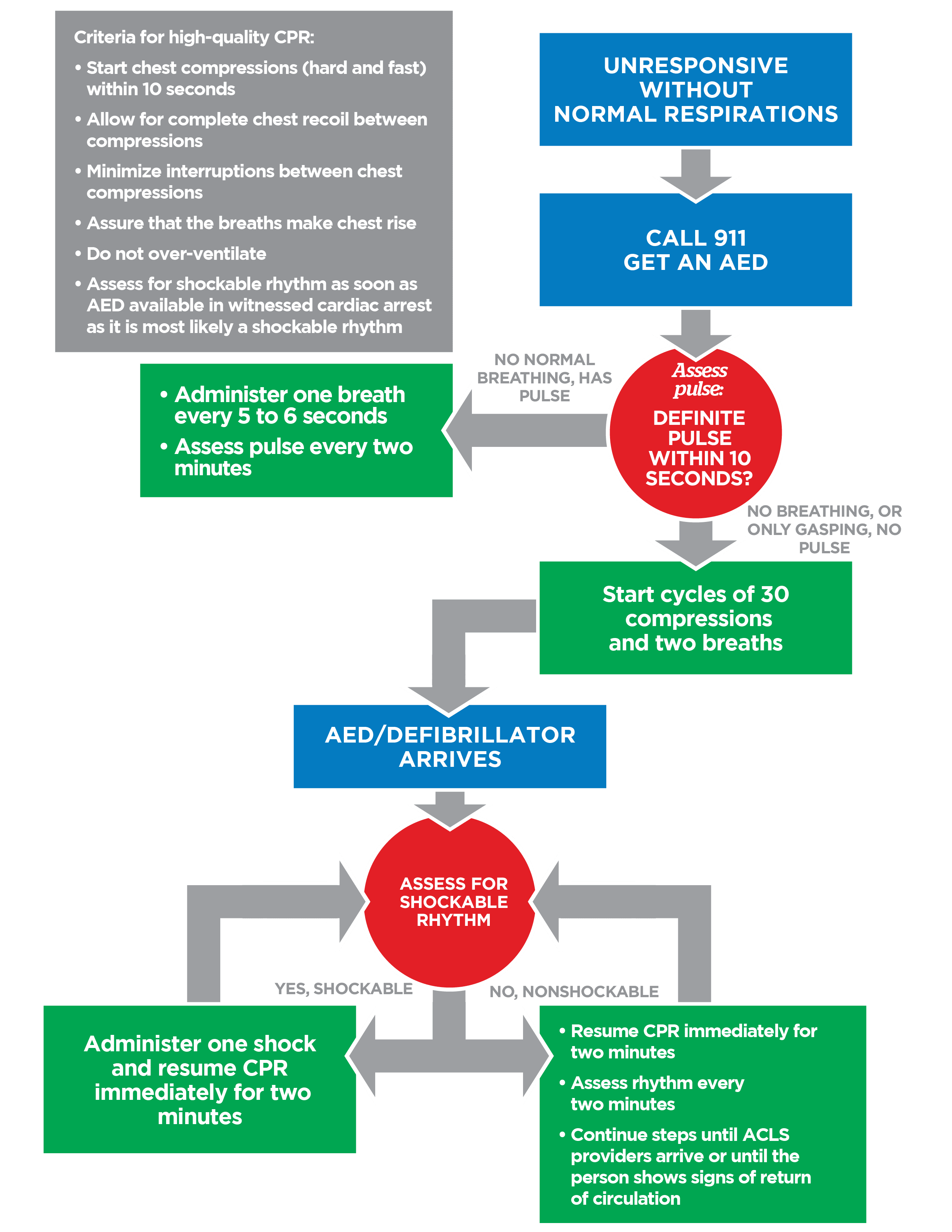
4. Adult BLS Algorithm (≥ 12 years)
Step 1: Scene Safety
- Ensure scene is safe for rescuer and victim
Step 2: Check Responsiveness
- Tap shoulders and shout: “Are you okay?”
Step 3: Activate Emergency Response
- Call emergency services
- Ask someone to bring an AED
Step 4: Check Breathing and Pulse (≤10 seconds)
- Check carotid pulse
- Look for normal breathing (gasping = not normal)
5. High-Quality CPR (Adults)
Chest Compressions
- Rate: 100–120/min
- Depth: 5–6 cm (2–2.4 inches)
- Hand position: Center of chest (lower half of sternum)
- Allow full chest recoil
- Minimize interruptions
Ventilation
- Compression : Ventilation ratio
* Single rescuer: 30 : 2
* Two rescuers: 30 : 2
- Each breath over 1 second
- Avoid excessive ventilation
6. Use of Automated External Defibrillator (AED)
- Turn on AED immediately when available
- Attach pads correctly
- Follow AED prompts
- Ensure no one touches patient during shock
- Resume CPR immediately after shock or “no shock advised”
7. Pediatric BLS (Children 1 year to puberty)
Key Differences
- Pulse check: Carotid or femoral
- Compression depth: ~5 cm (2 inches) or ⅓ chest depth
- Compression–Ventilation Ratio
* Single rescuer: 30 : 2
* Two rescuers: 15 : 2
8. Infant BLS (< 1 year)
Pulse Check
- Brachial pulse
Chest Compressions
- Two fingers (single rescuer)
- Two-thumb encircling technique (two rescuers)
- Depth: ~4 cm (1.5 inches)
Compression–Ventilation Ratio
- Single rescuer: 30 : 2
- Two rescuers: 15 : 2
9. Airway Obstruction (Choking)
Conscious Adult/Child
- Ask: “Are you choking?”
- Perform abdominal thrusts (Heimlich maneuver)
Pregnant or Obese
- Chest thrusts instead of abdominal thrusts
Unconscious Victim
- Start CPR
- Check mouth for visible foreign body before ventilation
- Do not blind finger sweep
10. Rescue Breathing (Pulse Present, No Breathing)
Adults
- 1 breath every 5–6 seconds (10–12/min)
Children & Infants
- 1 breath every 3–5 seconds (12–20/min)
11. Special Situations
- Drowning: Start with rescue breaths
- Trauma: Stabilize cervical spine
- Hypothermia: Continue CPR until rewarmed
- Opioid overdose: Give naloxone if available, continue CPR
12. Termination of BLS
Stop CPR only if:
- Victim shows signs of life
- Advanced care takes over
- Rescuer is exhausted
- Scene becomes unsafe
- Valid DNR order is present
13. Complications of CPR
- Rib fractures
- Sternal fractures
- Gastric distension
- Aspiration (rare compared to benefit)
14. Key Principles of Effective BLS
- Push hard and fast
- Minimize pauses
- Early defibrillation saves lives
- Good CPR is more important than ventilation initially
- Team coordination improves outcomes
15. Summary Table
| Component | Adults | Children | Infants |
| ------------------ | ----------- | --------------- | ----------- |
| Compression Rate | 100–120/min | 100–120/min | 100–120/min |
| Compression Depth | 5–6 cm | 5 cm | 4 cm |
| Ratio (1 rescuer) | 30:2 | 30:2 | 30:2 |
| Ratio (2 rescuers) | 30:2 | 15:2 | 15:2 |
| Pulse Check | Carotid | Carotid/Femoral | Brachial |
Clinical Pearl
> High-quality chest compressions and early defibrillation are the most critical determinants of survival in cardiac arrest.