1. Bony Pelvis (Pelvic Osteology)
Components
- Two hip bones (ilium, ischium, pubis)
- Sacrum
- Coccyx
Pelvic Types (Caldwell–Moloy)
- Gynecoid – Ideal for vaginal delivery
- Android – Funnel-shaped, obstructed labour risk
- Anthropoid – AP diameter longer
- Platypelloid – Flat pelvis, transverse diameter larger
Applied Importance
- Pelvimetry in obstructed labour
- Sacral promontory palpable in contracted pelvis
- Ischial spines → landmark for station of fetal head
- Coccyx injury during childbirth
- Pudendal nerve block near ischial spine
2. Pelvic Floor & Perineum
Muscles
- Levator ani (pubococcygeus, puborectalis, iliococcygeus)
- Coccygeus
- Perineal body (central tendon)
Applied Importance
- Weakness → uterine prolapse
- Injury during childbirth → cystocele, rectocele
- Episiotomy types:
* Midline
* Mediolateral (preferred in India)
- Perineal body damage → pelvic organ prolapse
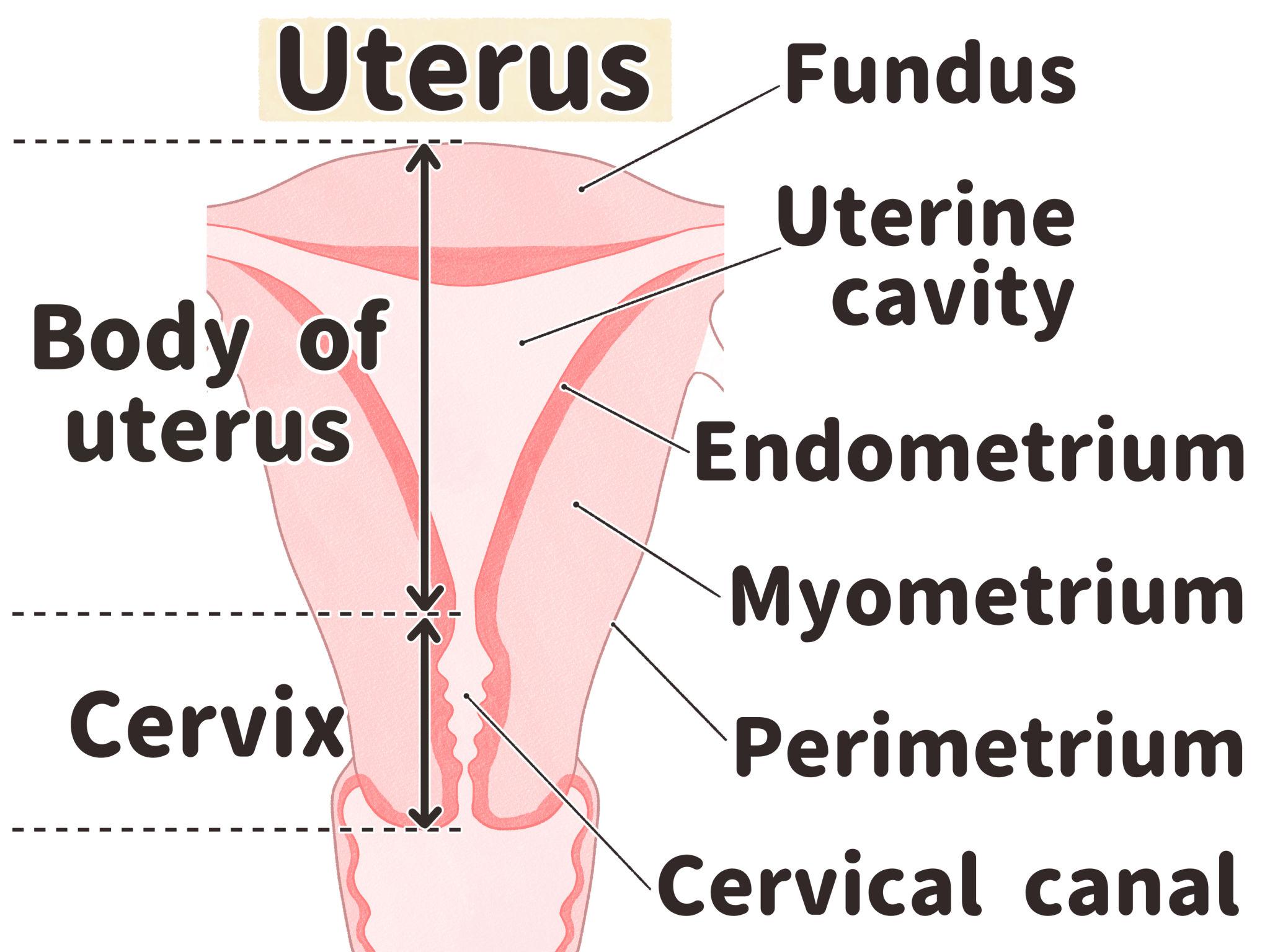
3. Uterus
Normal Anatomy
- Length: 7–8 cm
- Position: Anteverted & anteflexed
- Parts:
* Fundus
* Body
* Isthmus
* Cervix
Ligaments (Supports)
Primary Supports
- Transverse cervical (Cardinal)
- Uterosacral
- Pubocervical
Secondary Supports
- Round ligament
- Broad ligament
Blood Supply
- Uterine artery (from internal iliac)
- Anastomoses with ovarian artery
Applied Importance
- Hysterectomy → ureter lies under uterine artery ("water under bridge")
- Fibroids commonly in body
- Isthmus forms lower uterine segment in pregnancy
- Retroverted uterus → dyspareunia, backache
- Adenomyosis → thickened uterus
- Uterine rupture risk in scarred uterus
4. Cervix
Parts
- Ectocervix
- Endocervix
- Transformation zone (squamocolumnar junction)
Applied Importance
- Most cervical cancers arise at transformation zone
- Pap smear site
- Cervical incompetence → mid-trimester abortion
- Cone biopsy risk → cervical stenosis
5. Fallopian Tubes
Parts
- Interstitial
- Isthmus
- Ampulla (fertilization site)
- Infundibulum
Applied Importance
- Ectopic pregnancy common in ampulla
- Tubal ligation site → isthmus
- PID → hydrosalpinx
- Tubal block → infertility
6. Ovaries
Anatomy
- Almond-shaped
- Attached via:
* Ovarian ligament
* Suspensory ligament (infundibulopelvic ligament)
Blood Supply
- Ovarian artery (from aorta)
Applied Importance
- Ovarian torsion → acute abdomen
- PCOS → enlarged ovaries
- Ovarian tumors spread to peritoneum
- High vascularity → risk of hemorrhage during surgery
7. Broad Ligament
Double layer of peritoneum containing:
- Fallopian tube
- Ovarian ligament
- Uterine vessels
- Ureter nearby
Applied Importance
- Broad ligament hematoma
- Ectopic pregnancy may rupture into broad ligament
- Surgical landmark during hysterectomy
8. Urinary Bladder (Relation to Gynaecology)
- Lies anterior to uterus
- Separated by vesicouterine pouch
Applied Importance
- Bladder injury during:
* Caesarean section
* Hysterectomy
- Vesicovaginal fistula (VVF)
- Stress urinary incontinence → pelvic floor weakness
9. Ureter
- Crosses under uterine artery
- Close to cervix
Applied Importance
- Risk of injury in:
* Hysterectomy
* Radical hysterectomy
- Hydronephrosis in cervical cancer
10. Rectum
- Posterior to vagina
- Rectouterine pouch (Pouch of Douglas)
Applied Importance
- Culdocentesis
- Endometriosis deposits
- Rectocele
11. Blood Supply of Female Pelvis
Arteries
- Internal iliac artery branches:
* Uterine
* Vaginal
* Internal pudendal
Applied Importance
- Postpartum hemorrhage → uterine artery ligation
- Internal iliac ligation to control bleeding
- Pelvic congestion syndrome
12. Lymphatic Drainage (Very Important in Oncology)
Uterus
- Fundus → para-aortic nodes
- Body → external iliac
- Cervix → internal iliac & sacral
Ovary
- Para-aortic nodes
Applied Importance
- Staging of cervical cancer
- Radical hysterectomy includes node dissection
- Ovarian cancer spreads early via lymphatics
13. Nerve Supply
Autonomic
- Sympathetic (T10–L2)
- Parasympathetic (S2–S4)
Applied Importance
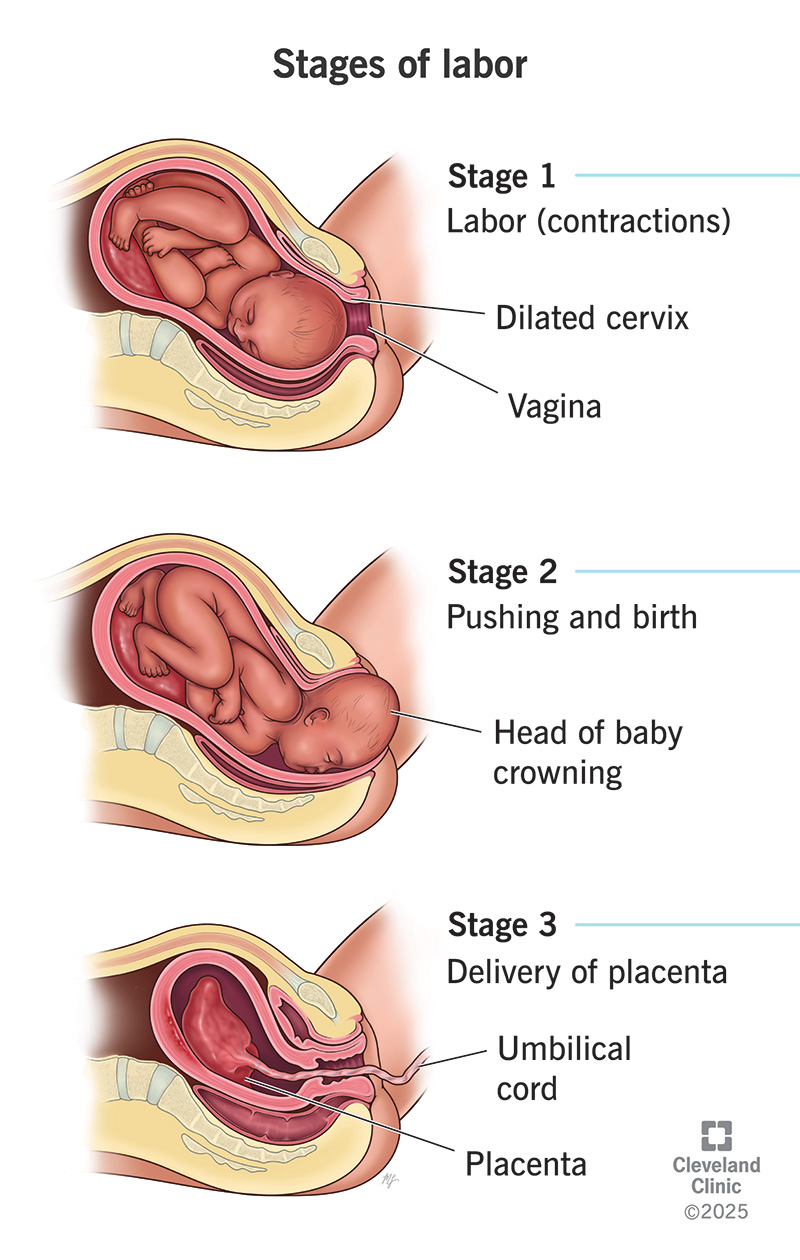
- Labour pain pathways:
* 1st stage → T10–L1
* 2nd stage → S2–S4
- Pudendal nerve block in labour
- Chronic pelvic pain syndromes
14. Vagina
Features
- Stratified squamous epithelium
- No glands
- Rich venous plexus
Applied Importance
- Site of delivery
- Vaginal hysterectomy route
- Bartholin cyst (at 4 & 8 o’clock)
- Vaginal carcinoma (rare)
15. Peritoneal Reflections
- Vesicouterine pouch
- Pouch of Douglas (deepest point in female pelvis)
Applied Importance
- Fluid collection in ectopic rupture
- Culdocentesis diagnostic test
- Endometriosis implants
16. Applied Anatomy in Common Surgeries
Hysterectomy
- Identify ureter
- Ligate uterine artery carefully
- Preserve ovarian blood supply if needed
Caesarean Section
- Incision through:
* Skin
* Rectus sheath
* Peritoneum
* Lower uterine segment
Tubal Ligation
- Identify isthmic portion
17. Applied Anatomy in Infertility
- Tubal patency
- Endometrial thickness
- Ovarian reserve
- Uterine anomalies (septate uterus)
18. Applied Anatomy in Prolapse
- Failure of:
* Cardinal ligament
* Uterosacral ligament
* Pelvic floor muscles
Degrees:
- 1st degree – descent
- 2nd degree – at introitus
- 3rd degree – complete prolapse
19. Developmental Anatomy (Important for Viva)
- Müllerian ducts form:
* Uterus
* Fallopian tubes
* Upper vagina
- Anomalies:
* Septate uterus
* Bicornuate uterus
* Unicornuate uterus
High-Yield Viva Points
- “Water under the bridge” → ureter under uterine artery
- Ampulla → fertilization site
- Transformation zone → cervical cancer site
- Pouch of Douglas → lowest peritoneal point
- Para-aortic nodes → ovarian cancer spread