Postpartum Hemorrhage Clinical Guide Causes Diagnosis and Management
Definition
Postpartum hemorrhage (PPH) is excessive bleeding after childbirth.
- Primary (early) PPH: ≥500 mL after vaginal delivery or ≥1000 mL after cesarean section within 24 hours
- Secondary (late) PPH: Excessive bleeding from 24 hours to 6 weeks postpartum
Epidemiology and Importance
- Leading cause of maternal mortality worldwide
- Rapid onset and progression require early recognition and protocol-based management
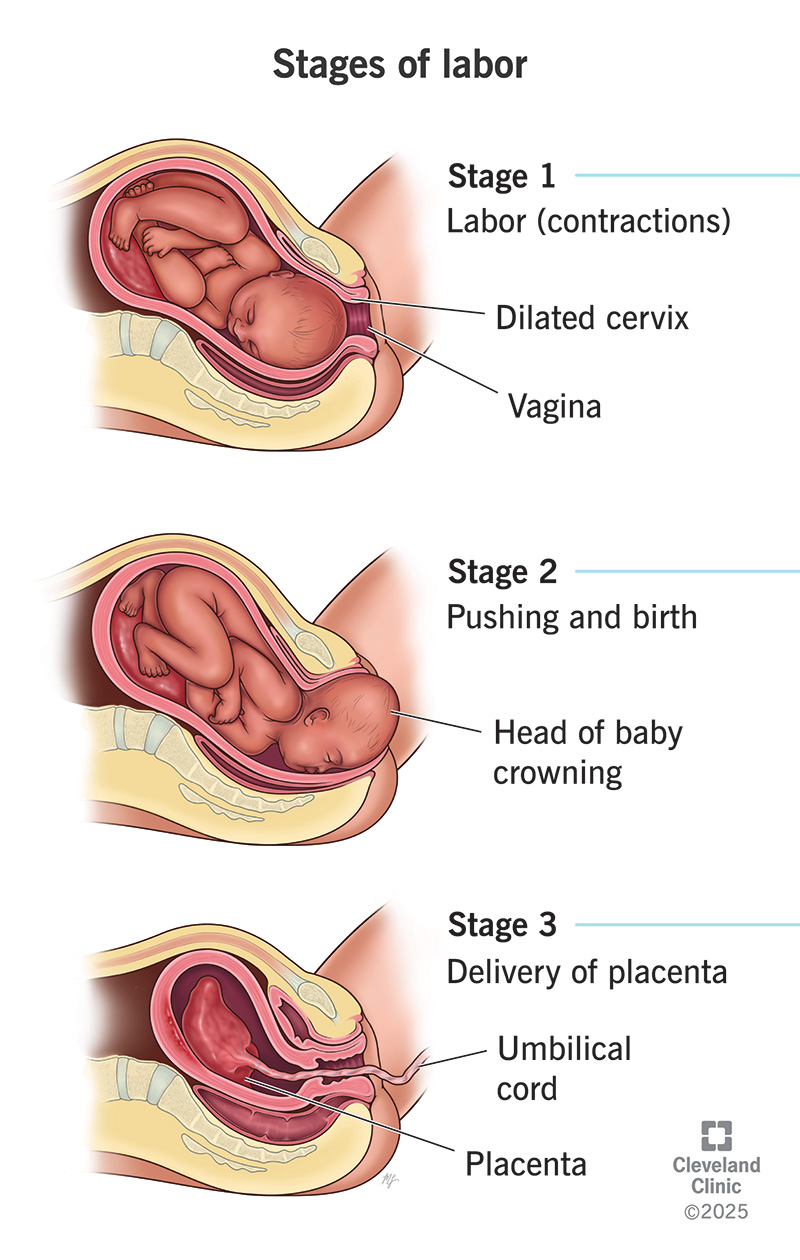
Pathophysiology
Normal hemostasis after delivery depends on uterine contraction compressing spiral arteries. Failure of contraction or disruption of clotting leads to uncontrolled bleeding.
Causes – “4 Ts” Framework
- Tone (most common – uterine atony)
* Overdistended uterus (multiple pregnancy, polyhydramnios, macrosomia)
* Prolonged or precipitous labor
* Chorioamnionitis
- Trauma
* Cervical, vaginal, perineal tears
* Uterine rupture
* Hematomas
- Tissue
* Retained placental tissue
* Placenta accreta spectrum
- Thrombin
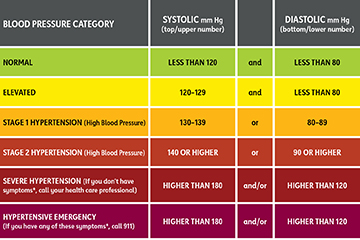
* Coagulopathies (DIC, severe preeclampsia, HELLP, anticoagulant use)
Risk Factors
- Previous PPH
- Operative delivery
- Induction or augmentation of labor
- Anemia
- Placenta previa or accreta
Clinical Features
- Excessive vaginal bleeding
- Boggy or enlarged uterus
- Signs of hypovolemia: tachycardia, hypotension, pallor, altered sensorium
- Reduced urine output
Initial Assessment and Diagnosis
Diagnosis is clinical and urgent
- Quantify blood loss (visual + weighing)
- Assess uterine tone
- Inspect birth canal
- Evaluate placenta completeness
Investigations (do not delay treatment)
- CBC (Hb, platelets)
- Blood group and cross-match
- Coagulation profile (PT, aPTT, fibrinogen)
- ABG if severe shock
Management – Stepwise Approach
Immediate Resuscitation
- Call for help
- Airway and oxygen
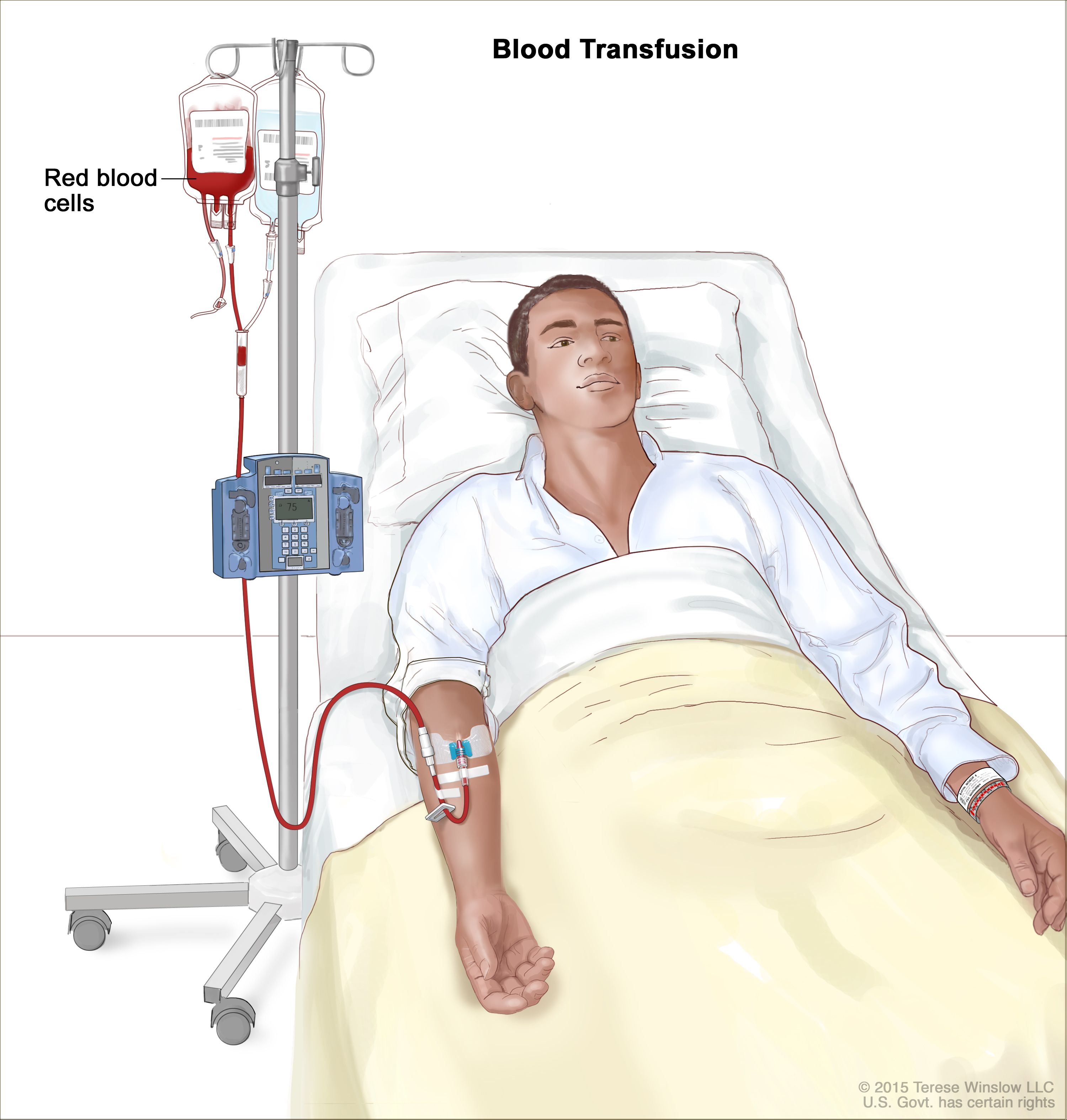
- Two wide-bore IV lines
- Crystalloids followed by blood products (1:1:1 PRBC:plasma:platelets if massive)
Uterotonic Drugs (Cornerstone of Treatment)
1. Oxytocin
- Indication: First-line for uterine atony
- Mechanism: Stimulates uterine smooth muscle contraction
- Dose:
* IV infusion: 10–40 IU in 1 L NS/RL
* IM: 10 IU
- Adverse effects: Hypotension (rapid IV), water intoxication
- Contraindications: None significant in PPH
- Monitoring: Uterine tone, vitals
- Counselling: First-line and safe
2. Methylergometrine
- Mechanism: Sustained uterine contraction via alpha-adrenergic stimulation
- Dose: 0.2 mg IM (may repeat)
- Adverse effects: Hypertension, nausea
- Contraindications: Hypertension, preeclampsia, cardiac disease
- Monitoring: Blood pressure
3. Carboprost (15-methyl PGF2α)
- Mechanism: Prostaglandin-induced myometrial contraction
- Dose: 250 µg IM every 15–90 min (max 8 doses)
- Adverse effects: Bronchospasm, diarrhea, fever
- Contraindications: Asthma
- Monitoring: Respiratory status
4. Misoprostol
- Mechanism: Prostaglandin E1 analog
- Dose: 800–1000 µg rectal or sublingual
- Adverse effects: Fever, shivering
- Use: Low-resource settings
5. Tranexamic Acid
- Indication: All PPH within 3 hours of onset
- Mechanism: Inhibits fibrinolysis
- Dose: 1 g IV over 10 min (repeat once if bleeding continues)
- Adverse effects: Rare thrombosis
- Contraindications: Active thromboembolic disease
- Monitoring: Renal function if repeated
- Counselling: Reduces mortality when given early
Mechanical and Surgical Measures
Mechanical
- Bimanual uterine massage
- Uterine balloon tamponade (Bakri balloon)
- Uterine packing
Surgical
- Uterine compression sutures (B-Lynch)
- Uterine artery ligation
- Internal iliac artery ligation
- Hysterectomy (life-saving last resort)
Management by Cause
- Atony: Uterotonics → balloon → surgery
- Trauma: Immediate repair of tears
- Tissue: Manual removal, curettage
- Thrombin: Correct coagulopathy with blood products
Secondary Postpartum Hemorrhage
Causes
- Retained products
- Subinvolution of uterus
- Endometritis
Management
- Antibiotics
- Uterotonics
- Ultrasound-guided evacuation if indicated
Complications
- Hypovolemic shock
- Acute kidney injury
- DIC
- Sheehan syndrome
- Maternal death
Prevention
- Active management of third stage of labor
- Antenatal anemia correction
- Risk stratification and preparedness
Prognosis
Excellent with early recognition and protocol-driven care; delays increase morbidity and mortality.
SEO Meta Data
SEO Title:
Postpartum Hemorrhage Causes Diagnosis and Management
Meta Description:
Comprehensive clinical guide on postpartum hemorrhage covering causes, diagnosis, stepwise management, uterotonic drugs, surgical options, prevention, and complications.
SEO Keywords (comma separated):
postpartum hemorrhage, PPH management, uterine atony, causes of PPH, tranexamic acid PPH, obstetric emergency, maternal hemorrhage, third stage labor complications
Frequently Asked Questions
What is the most common cause of postpartum hemorrhage?
Uterine atony.
When should tranexamic acid be given in PPH?
Within 3 hours of onset of bleeding.
What is the first-line drug for PPH?
Oxytocin.
When is hysterectomy indicated in PPH?
When bleeding is uncontrollable and life-threatening despite conservative measures.
Can PPH occur after 24 hours?
Yes, it is termed secondary postpartum hemorrhage.