Malpresentation in Obstetrics
Definition
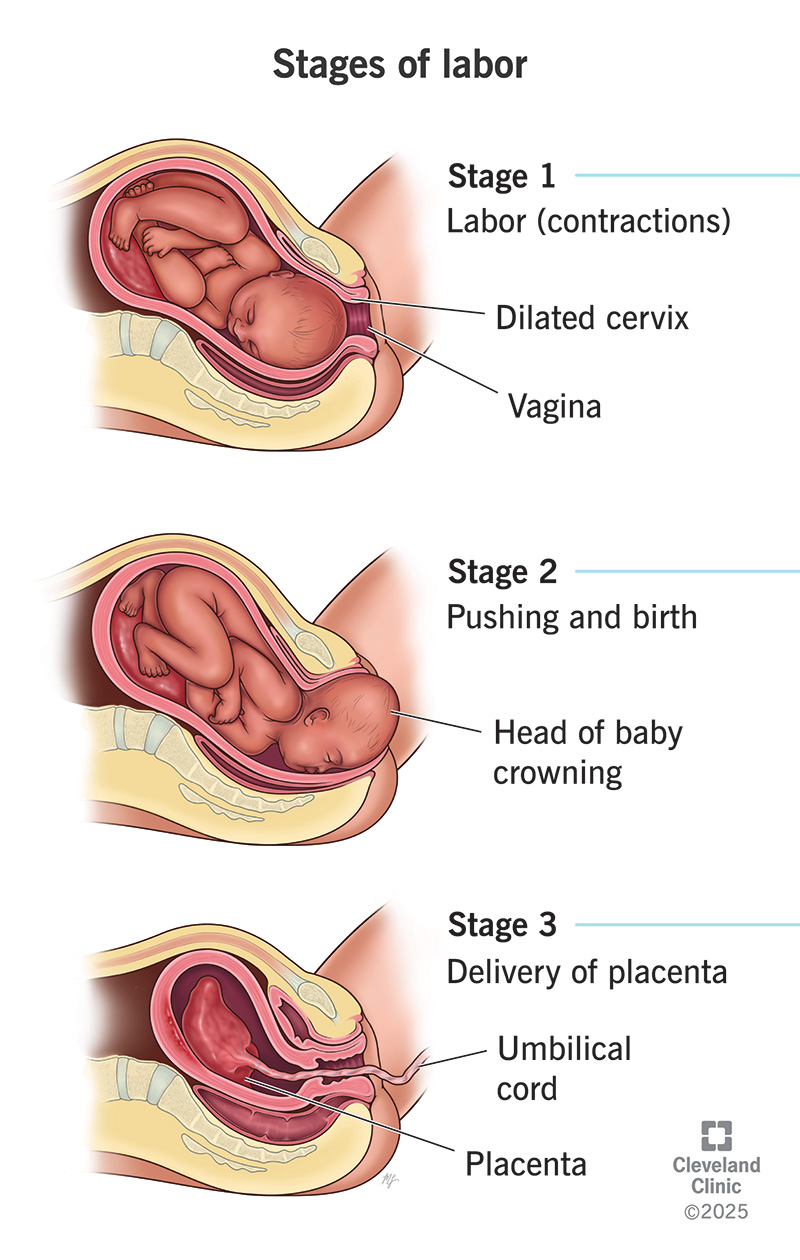
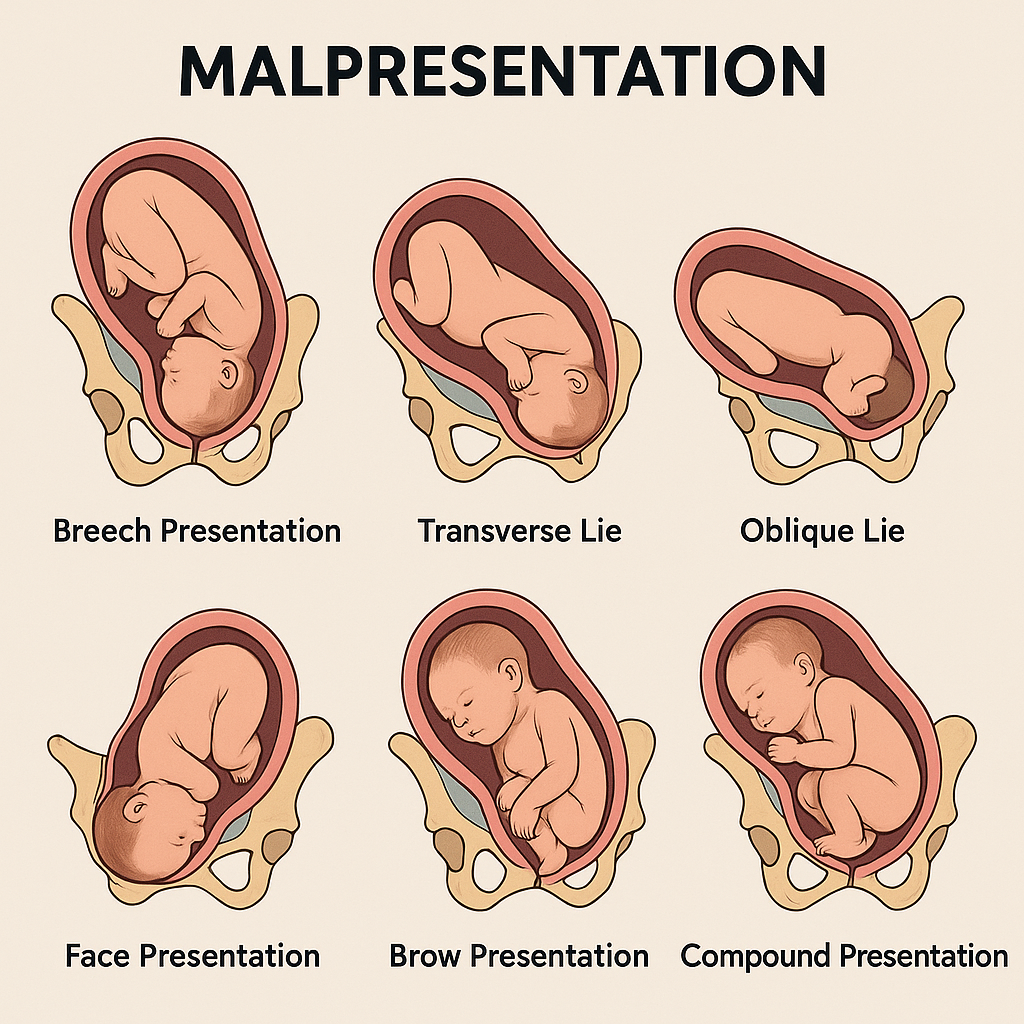
Malpresentation refers to any fetal presentation other than the normal vertex (cephalic, occiput-anterior) at the time of labor or delivery. It includes breech, transverse, oblique, face, brow, and compound presentations and is a major cause of obstructed labor, operative delivery, and perinatal morbidity.
Classification of Malpresentation
1. Breech Presentation (≈3–4% at term)
- Frank breech: Hips flexed, knees extended (most common)
- Complete breech: Hips and knees flexed
- Footling breech: One or both feet present first
2. Transverse Lie
- Fetal long axis perpendicular to maternal spine
- Shoulder presentation
3. Oblique Lie
- Fetal axis oblique to maternal axis
- Unstable lie
4. Face Presentation
- Complete extension of fetal head
- Mentum (chin) is the denominator
5. Brow Presentation
- Partial extension of fetal head
- Largest presenting diameter (mento-vertical)
6. Compound Presentation
- Prolapse of an extremity alongside the presenting part (e.g., hand with head)
Etiology and Risk Factors
Maternal Factors
- Grand multiparity
- Uterine anomalies (bicornuate, septate uterus)
- Placenta previa
- Pelvic tumors or contracted pelvis
- Polyhydramnios
Fetal Factors
- Prematurity
- Multiple pregnancy
- Congenital anomalies (hydrocephalus, anencephaly)
- Fetal growth restriction
Placental Factors
- Placenta previa
- Fundal or cornual placentation
Pathophysiology (Why Malpresentation Occurs)
- Abnormal uterine shape or space prevents normal fetal flexion and rotation
- Excess or reduced amniotic fluid alters fetal mobility
- Fetal anomalies interfere with normal engagement
- Placental location obstructs the lower uterine segment
Clinical Features
Antenatal
- Abnormal lie or presentation on Leopold’s maneuvers
- Difficulty identifying fetal head in pelvis
- Irregular abdominal contour
Intrapartum
- Delayed labor progress
- Cord prolapse (especially breech, transverse lie)
- Abnormal presenting part on vaginal examination
Diagnosis
Clinical Examination
- Abdominal palpation: Leopold’s maneuvers
- Vaginal examination: Identification of presenting part landmarks
Imaging
- Ultrasound (gold standard)
* Confirms presentation, lie, fetal anomalies, placental position
- X-ray pelvis (obsolete, rarely used)
Management – Stepwise Approach
Antenatal Management
- External Cephalic Version (ECV)
* Indication: Breech at ≥36–37 weeks
* Contraindications: Placenta previa, multiple pregnancy (except second twin), uterine scar with risk, fetal compromise
* Success rate: ~50–60%
- Monitoring and Counseling
* Mode of delivery planning
* Institutional delivery mandatory
Intrapartum Management (According to Type)
Breech Presentation
- Planned vaginal breech delivery (selected cases only):
* Frank or complete breech
* Adequate pelvis
* Estimated fetal weight 2.5–3.5 kg
* Experienced obstetrician
- Elective cesarean section:
* Footling breech
* Large fetus
* Primigravida with breech
* Fetal distress
Transverse / Oblique Lie
- Cesarean section is mandatory
- Internal podalic version only for second twin (rare)
Face Presentation
- Mentum anterior → vaginal delivery possible
- Mentum posterior → cesarean section
Brow Presentation
- Persistent brow → cesarean section (vaginal delivery impossible)
Compound Presentation
- Usually converts spontaneously
- Cesarean if cord prolapse or obstruction
Complications
Maternal
- Obstructed labor
- Uterine rupture
- Postpartum hemorrhage
- Operative delivery complications
Fetal
- Birth asphyxia
- Cord prolapse
- Birth trauma (intracranial hemorrhage, fractures)
- Increased perinatal mortality
Prevention
- Early antenatal registration
- Routine third-trimester ultrasound
- Timely ECV
- Planned institutional delivery
Prognosis
- Good with early diagnosis and planned management
- Poor outcomes associated with delayed referral, home delivery, and unskilled handling
Key Clinical Pearls (Exam & Practice Oriented)
- Most common malpresentation at term: Breech
- Most dangerous malpresentation: Transverse lie
- Largest presenting diameter: Brow presentation
- Best investigation: Ultrasound