Complications of the Third Stage of Labour
Introduction
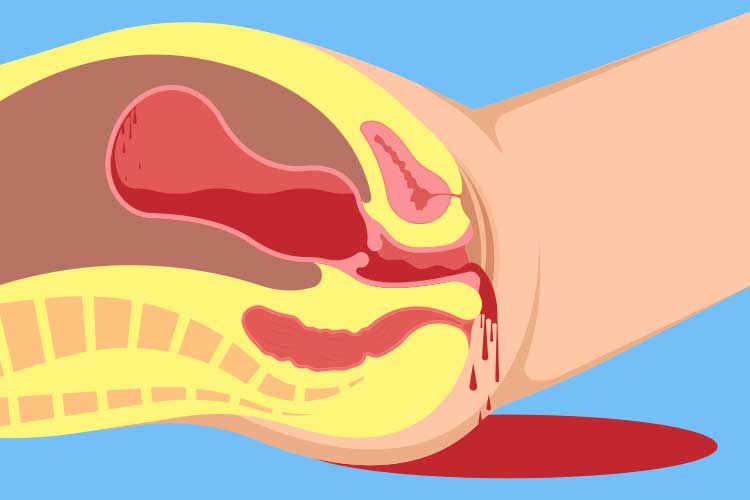
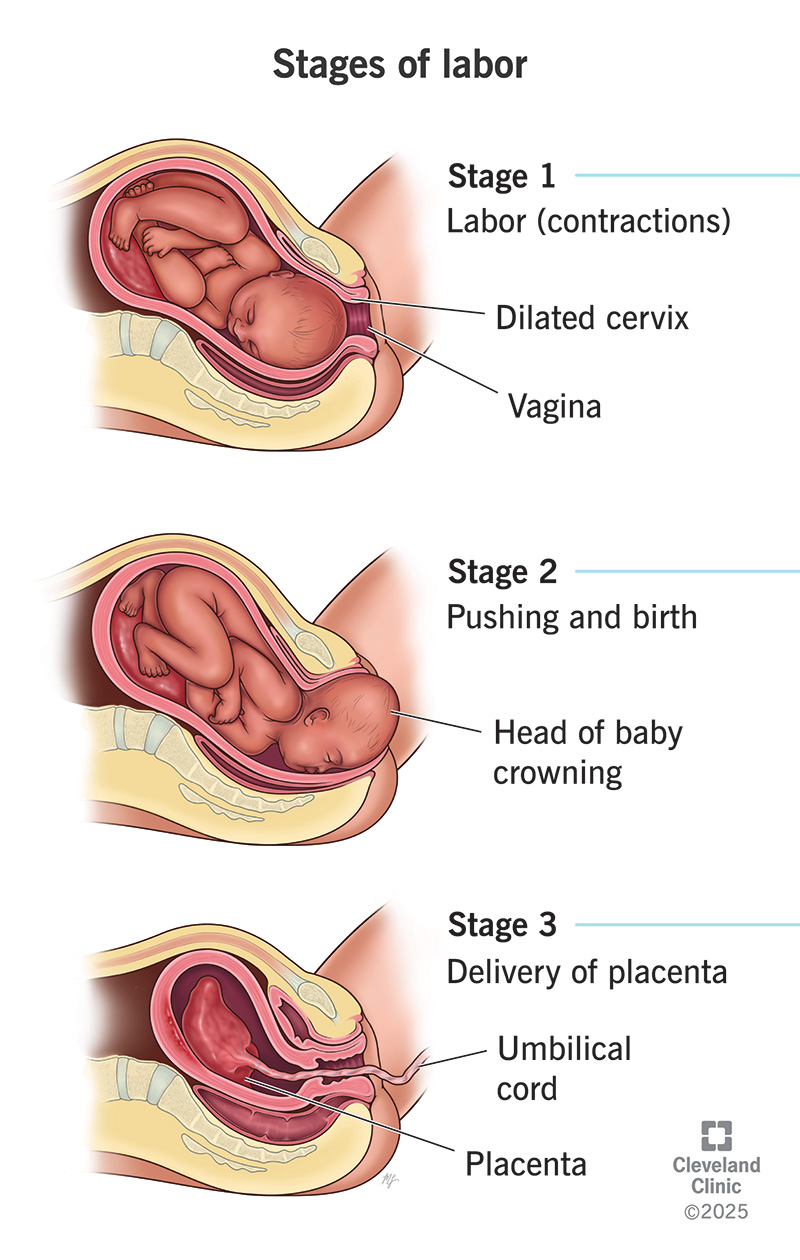
The third stage of labour begins after the birth of the baby and ends with complete expulsion of the placenta and membranes. Although usually short (5–30 minutes), this stage is high-risk because most cases of maternal morbidity and mortality occur here, mainly due to hemorrhage.
Major Complications of the Third Stage of Labour
1. Postpartum Hemorrhage (PPH)
Definition
Excessive bleeding after delivery:
- ≥ 500 mL after vaginal delivery
- ≥ 1000 mL after cesarean section
Causes (4 Ts)
- Tone – Uterine atony (most common)
- Tissue – Retained placenta or placental fragments
- Trauma – Genital tract tears, uterine rupture
- Thrombin – Coagulation disorders
Risk Factors
- Prolonged labour
- Overdistended uterus (multiple pregnancy, polyhydramnios)
- Induction or augmentation of labour
- Previous PPH
- Placenta previa or accreta
Clinical Features
- Heavy vaginal bleeding
- Boggy uterus
- Hypotension, tachycardia
- Pallor, shock
Prevention
- Active management of third stage of labour (AMTSL)
- Oxytocin 10 IU IM/IV
- Controlled cord traction
- Uterine massage
2. Retained Placenta
Definition
Failure of placenta expulsion within:
- 30 minutes (with active management)
- 60 minutes (with expectant management)
Types
- Placenta adherens
- Trapped placenta
- Placenta accreta spectrum
Complications
- Severe PPH
- Infection
- Uterine inversion (during traction)
Management
- Manual removal under anesthesia
- Uterotonics
- Antibiotic prophylaxis
3. Placenta Accreta Spectrum
Types
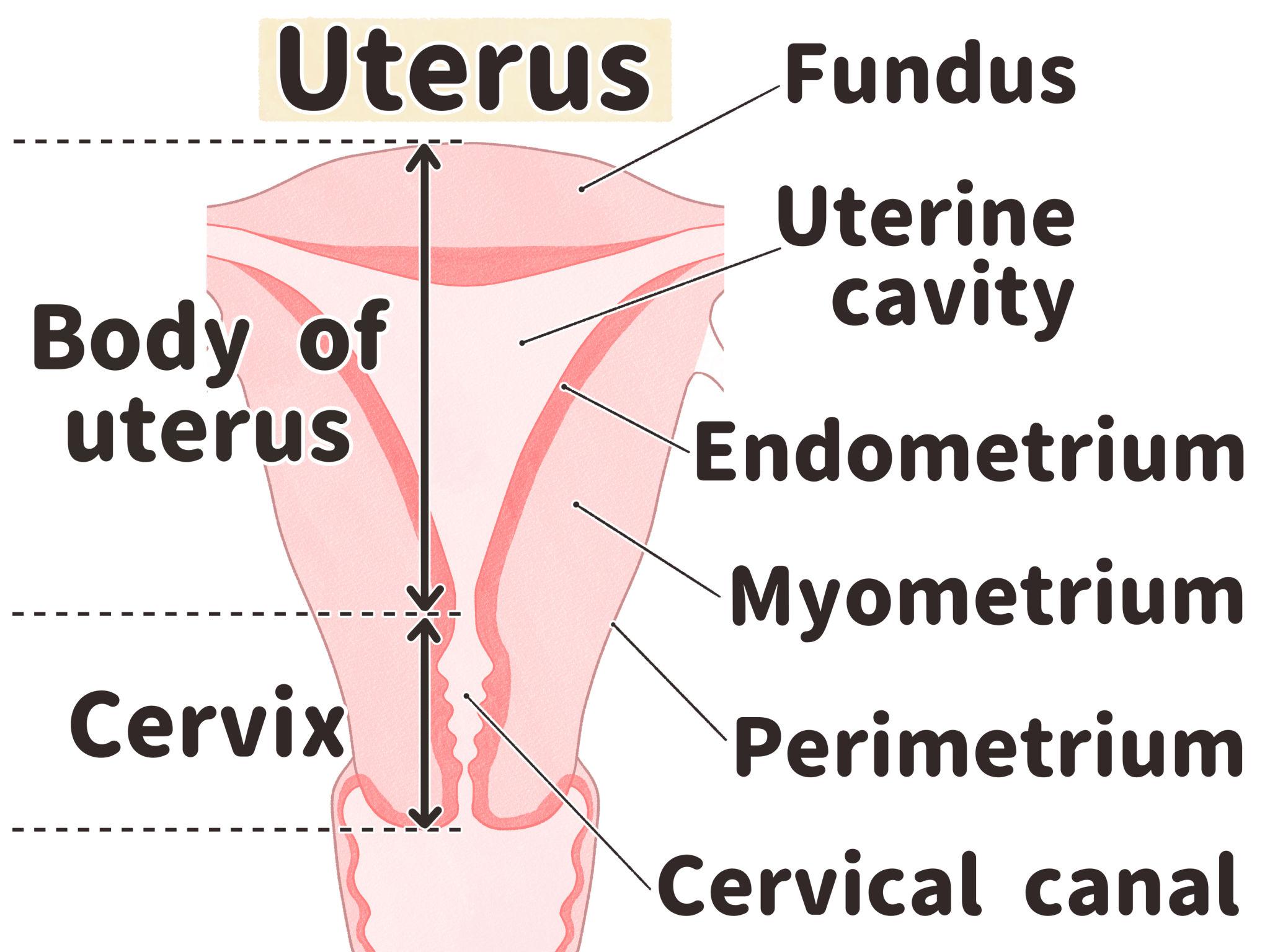
- Accreta – Placenta attached to myometrium
- Increta – Invades myometrium
- Percreta – Penetrates uterine serosa
Complications
- Massive hemorrhage
- Need for hysterectomy
- Maternal mortality
4. Uterine Inversion
Definition
Turning inside out of the uterus following delivery
Causes
- Excessive cord traction
- Fundal pressure before placental separation
- Adherent placenta
Clinical Features
- Sudden severe hemorrhage
- Shock out of proportion to blood loss
- Visible mass at introitus
Management
- Immediate manual reposition (Johnson maneuver)
- Tocolytics followed by uterotonics
5. Genital Tract Trauma
Types
- Cervical tears
- Vaginal tears
- Perineal tears
Risk Factors
- Instrumental delivery
- Precipitous labour
- Large baby
Complications
- Persistent bleeding despite well-contracted uterus
- Hematoma formation
6. Puerperal Infection
Causes
- Retained products of conception
- Prolonged third stage
- Unsterile manual placental removal
Clinical Features
- Fever
- Foul-smelling lochia
- Uterine tenderness
7. Amniotic Fluid Embolism (Rare but Fatal)
Features
- Sudden respiratory distress
- Hypotension
- Disseminated intravascular coagulation (DIC)
8. Shock
Types
- Hemorrhagic shock
- Neurogenic shock (uterine inversion)
- Septic shock
Prevention of Complications
- Active management of third stage of labour
- Skilled birth attendance
- Early identification of high-risk pregnancies
- Availability of blood transfusion services
Key Points for Exams and Clinical Practice
- Uterine atony is the most common cause of PPH
- AMTSL reduces PPH by more than 60%
- Persistent bleeding with firm uterus suggests trauma
- Retained placenta increases risk of PPH and infection