Malnutrition in Paediatrics (Childhood Malnutrition)
1. Definition
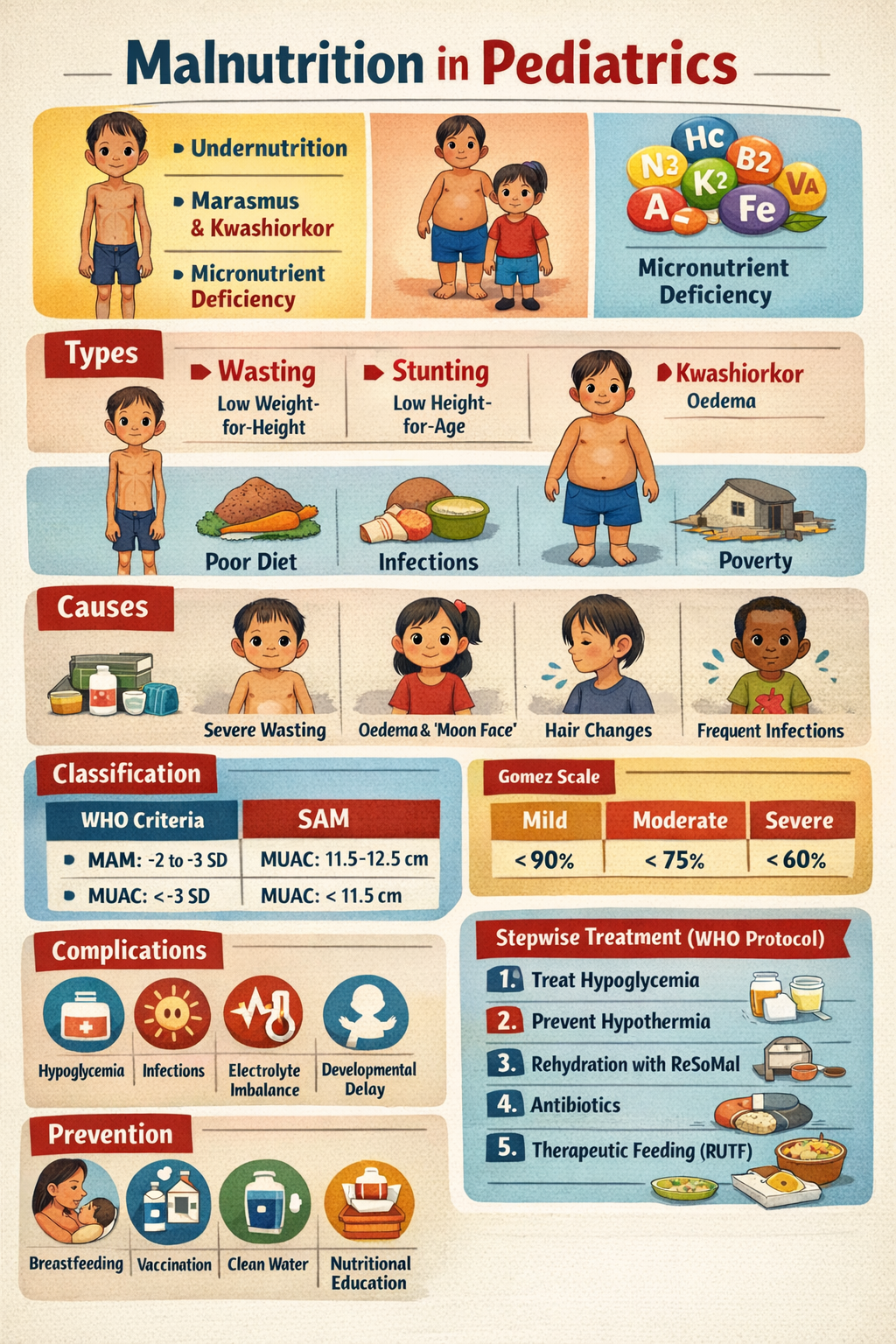
Malnutrition in paediatrics refers to an imbalance between the body’s nutritional requirements and nutrient intake, resulting in deficiency, excess, or improper utilization of nutrients. In children it most commonly refers to undernutrition, which includes:
- Underweight – low weight for age
- Stunting – low height for age (chronic malnutrition)
- Wasting – low weight for height (acute malnutrition)
Severe forms include Severe Acute Malnutrition (SAM) such as Marasmus and Kwashiorkor.
2. Pathophysiology
Malnutrition results from inadequate intake, impaired absorption, increased metabolic demand, or nutrient loss.
Mechanism
- Insufficient energy intake
* Depletion of glycogen stores
* Fat breakdown (lipolysis)
- Protein deficiency
* Muscle wasting
* Reduced plasma proteins (albumin)
* Edema due to decreased oncotic pressure
- Micronutrient deficiency
* Impaired immunity
* Delayed growth and development
- Metabolic adaptation
* Reduced basal metabolic rate
* Hormonal changes (↓ insulin, ↑ cortisol)
- Immune dysfunction
* Increased susceptibility to infections
3. Causes / Risk Factors
A. Inadequate Intake
- Poor breastfeeding practices
- Improper complementary feeding
- Food insecurity or poverty
- Neglect or poor caregiving
B. Increased Nutritional Requirements
- Chronic infections
- Congenital heart disease
- Chronic lung disease
- Malignancy
C. Malabsorption
- Celiac disease
- Chronic diarrhea
- Cystic fibrosis
- Short bowel syndrome
D. Increased Nutrient Loss
- Persistent diarrhea
- Nephrotic syndrome
- Burns
E. Socioeconomic Factors
- Poor sanitation
- Large family size
- Lack of health education
- Inadequate maternal nutrition
4. Types of Malnutrition
1. Marasmus
Severe calorie deficiency.
Features
- Severe wasting
- Loss of subcutaneous fat
- Prominent ribs
- “Old man” appearance
- No edema
- Irritable but alert
2. Kwashiorkor
Severe protein deficiency with relatively adequate calories.
Features
- Edema
- Fatty liver
- Moon face
- Dermatitis (flaky paint appearance)
- Hair changes (flag sign)
- Apathy
3. Marasmic Kwashiorkor
Combination of wasting and edema.
5. Clinical Features
General Signs
- Poor weight gain
- Growth retardation
- Weakness
- Irritability
- Delayed developmental milestones
Physical Findings
- Muscle wasting
- Thin limbs
- Dry skin
- Sparse hair
- Enlarged liver (kwashiorkor)
Severe Acute Malnutrition Signs
- Bilateral pitting edema
- Weight-for-height < −3 SD
- MUAC < 11.5 cm (6–59 months)
Systemic Effects
- Frequent infections
- Hypothermia
- Hypoglycemia
- Anemia
- Delayed wound healing
6. Investigations / Diagnosis
Anthropometric Measurements
- Weight-for-age
- Height-for-age
- Weight-for-height
- Mid Upper Arm Circumference (MUAC)
- BMI-for-age
WHO Criteria for Severe Acute Malnutrition
Any one of the following:
- Weight-for-height < −3 SD
- MUAC < 11.5 cm
- Bilateral pitting edema
Laboratory Investigations
- Complete blood count → anemia
- Serum albumin ↓
- Blood glucose ↓
- Electrolyte imbalance
- Liver function tests
- Stool examination (parasites)
7. Differential Diagnosis
Conditions that mimic malnutrition:
- Celiac disease
- Congenital heart disease
- Chronic infections (TB, HIV)
- Metabolic disorders
- Endocrine disorders
* Hypothyroidism
* Growth hormone deficiency
8. Management
Management depends on severity.
A. Severe Acute Malnutrition (SAM)
WHO management follows 10-step protocol.
Step 1: Treat Hypoglycemia
Give 10% glucose or oral sugar solution.
Step 2: Treat Hypothermia
Keep child warm
Skin-to-skin care.
Step 3: Treat Dehydration
Use ReSoMal (Rehydration Solution for Malnutrition).
Step 4: Correct Electrolyte Imbalance
Common deficiencies:
- Potassium
- Magnesium
Step 5: Treat Infection
Children with SAM are assumed to have infection.
Common antibiotics:
- Ampicillin
- Gentamicin
Drug Details
Ampicillin
Indication
Empirical treatment of infection in severe malnutrition.
Mechanism of Action
Beta-lactam antibiotic that inhibits bacterial cell wall synthesis.
Usual Dose
- Children: 50 mg/kg IV every 6 hours
Pharmacokinetics
- Good tissue penetration
- Renal excretion
Adverse Effects
- Rash
- Diarrhea
- Hypersensitivity reactions
Contraindications
- Penicillin allergy
Drug Interactions
- Reduced effect with bacteriostatic antibiotics
Monitoring
- Signs of allergic reaction
- Renal function
Patient Counselling
- Complete antibiotic course
- Report rash or breathing difficulty.
Gentamicin
Indication
Severe gram-negative infections in SAM.
Mechanism
Binds 30S ribosomal subunit, inhibiting bacterial protein synthesis.
Dose
- 7.5 mg/kg/day IV or IM
Pharmacokinetics
- Poor oral absorption
- Renal elimination
Adverse Effects
- Nephrotoxicity
- Ototoxicity
Contraindications
- Severe renal impairment
Drug Interactions
- Increased toxicity with loop diuretics
Monitoring
- Renal function
- Hearing
Counselling
- Report hearing problems or reduced urine output.
9. Nutritional Rehabilitation
Stabilization Phase
Use F-75 therapeutic milk
- 75 kcal / 100 ml
- Low protein and sodium
Rehabilitation Phase
Use F-100 therapeutic milk
- 100 kcal / 100 ml
- Higher protein
Ready-to-Use Therapeutic Food (RUTF)
Example:
- Peanut-based paste
- High calorie
10. Micronutrient Supplementation
Important supplements:
- Vitamin A
- Folic acid
- Zinc
- Iron (after stabilization)
11. Non-Pharmacological Management
- Early breastfeeding
- Proper complementary feeding
- Nutritional education of parents
- Hygiene and sanitation
- Immunization
- Growth monitoring
12. Complications
Untreated malnutrition may cause:
- Severe infections
- Developmental delay
- Cognitive impairment
- Organ failure
- Death
13. Prevention
Primary Prevention
- Exclusive breastfeeding for 6 months
- Adequate complementary feeding
- Maternal nutrition
- Food security
Secondary Prevention
- Growth monitoring
- Early detection of undernutrition
Community Programs
- ICDS
- Mid-day meal program
- Vitamin supplementation
14. Prognosis
Prognosis depends on:
- Severity of malnutrition
- Presence of infection
- Early treatment
With proper treatment most children recover completely, but severe cases may have long-term growth and cognitive deficits.
If you want, I can also give:
• Malnutrition classification (WHO, Gomez, Waterlow)
• MCQs for exams (NEET PG / MBBS / Nursing)
• Complete paediatric nutrition chart.