Abnormality of Stature (Growth Disorders) — Full Detail
1. Definition
Stature refers to a child’s height/length compared with age- and sex-matched norms.
Abnormal stature includes:
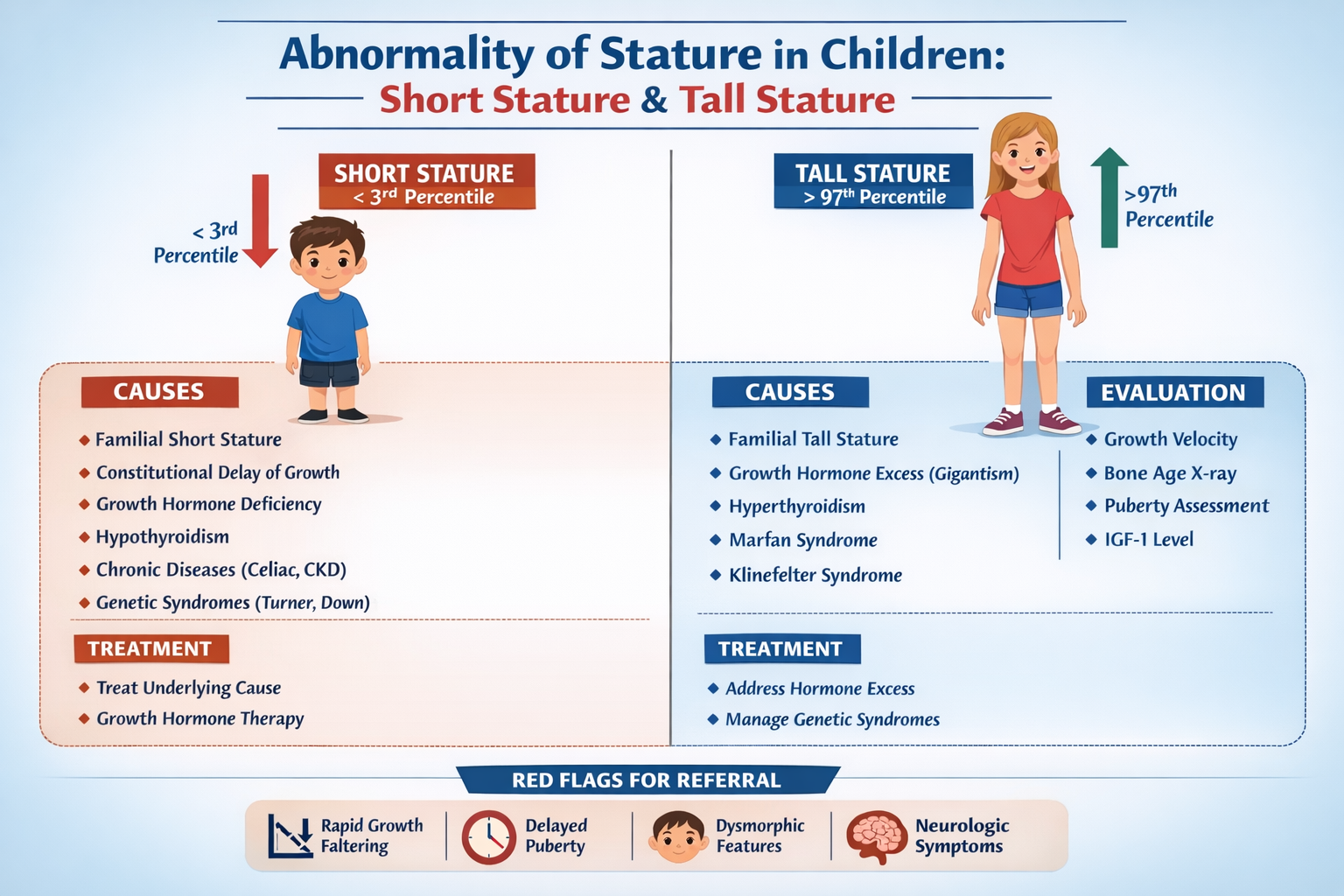
- Short stature: Height < –2 SD or below 3rd percentile
- Tall stature: Height > +2 SD or above 97th percentile
- Growth failure: Poor height velocity over time
2. Normal Growth Physiology
Growth depends on:
- Genetics
- Nutrition
- Endocrine hormones
* Growth hormone (GH)
* Thyroid hormone
* Sex steroids
- Chronic disease status
- Psychosocial environment
3. Classification of Abnormal Stature
A. Short Stature
- Normal variant
- Pathological causes
- Syndromic causes
B. Tall Stature
- Familial tall stature
- Endocrine excess
- Genetic syndromes
SHORT STATURE — COMPLETE DETAIL
4. Definition
Short stature is:
- Height < 3rd percentile OR
- Height < –2 SD for age/sex OR
- Growth velocity below expected
5. Causes of Short Stature
A. Normal Variants (Non-pathologic)
1. Familial Short Stature
- Parents are short
- Child grows normally along low percentile
- Bone age = chronological age
- Puberty normal
2. Constitutional Delay of Growth and Puberty (CDGP)
- Delayed puberty
- Bone age delayed
- Growth velocity normal
- Family history of “late bloomers”
B. Endocrine Causes
1. Growth Hormone Deficiency
- Poor growth velocity
- Increased fat mass
- Immature face
- Delayed bone age
2. Hypothyroidism
- Short stature with weight gain
- Lethargy, constipation
- Delayed bone age
3. Cushing Syndrome
- Growth failure with obesity
- Moon face, striae
C. Chronic Systemic Diseases
- Chronic kidney disease
- Congenital heart disease
- Malabsorption (celiac disease)
- Chronic infection (TB, HIV)
Clue: Weight affected before height
D. Malnutrition
- Commonest cause worldwide
- Both weight and height reduced
E. Genetic and Syndromic Causes
Turner Syndrome (Girls)
- Short stature
- Webbed neck
- Amenorrhea
- XO karyotype
Down Syndrome
- Short stature with dysmorphic features
Skeletal Dysplasias
- Achondroplasia (disproportionate short stature)
F. Intrauterine Growth Restriction (IUGR)
- Small for gestational age
- Failure of catch-up growth
6. Clinical Evaluation of Short Stature
History
- Birth weight/length
- Growth pattern since infancy
- Nutrition and feeding
- Chronic illness symptoms
- Family height history
- Puberty timing
Examination
- Accurate height measurement
- Body proportions:
* Upper segment/lower segment ratio
* Arm span
- Dysmorphic features
- Pubertal staging (Tanner)
- Signs of systemic disease
Growth Velocity
Normal height velocity:
- 0–1 yr: ~25 cm/year
- 1–2 yr: ~12 cm/year
- 2–4 yr: ~7 cm/year
- Childhood: 5–6 cm/year
- Puberty: 8–12 cm/year
7. Investigations
Baseline Tests
- CBC (anemia, chronic disease)
- ESR/CRP (inflammation)
- Renal and liver function
- Celiac screen (tTG IgA)
- Thyroid profile (TSH, FT4)
Bone Age
X-ray left hand/wrist:
- Delayed → endocrine/CDGP
- Normal → familial short stature
- Advanced → precocious puberty
Hormonal Tests
- IGF-1 and IGFBP-3
- GH stimulation test (if suspected deficiency)
Genetic Tests
- Karyotype in girls (Turner syndrome)
8. Management of Short Stature
A. Treat Underlying Cause
- Nutrition rehabilitation
- Treat chronic disease
- Thyroxine for hypothyroidism
- Gluten-free diet for celiac
B. Growth Hormone Therapy
Indications
- GH deficiency
- Turner syndrome
- Chronic renal failure
- Prader-Willi syndrome
- Idiopathic short stature (selected)
Drug: Somatropin (Recombinant GH)
- Mechanism: Stimulates IGF-1 → growth plate proliferation
- Dose: 0.025–0.05 mg/kg/day SC
- Adverse effects:
* Intracranial hypertension
* Slipped capital femoral epiphysis
* Hyperglycemia
- Monitoring:
* Growth velocity
* IGF-1 levels
* Thyroid function
C. Puberty Induction (CDGP severe cases)
- Low-dose testosterone (boys)
- Estrogen therapy (girls)
TALL STATURE — COMPLETE DETAIL
9. Definition
Tall stature:
- Height > 97th percentile or > +2 SD
10. Causes of Tall Stature
A. Normal Variants
Familial Tall Stature
- Parents tall
- Normal growth velocity
- Bone age normal/slightly advanced
B. Endocrine Causes
1. Growth Hormone Excess (Gigantism)
- Rapid growth velocity
- Coarse facial features
- Enlarged hands/feet
2. Hyperthyroidism
- Increased growth rate
- Weight loss, tremors
3. Precocious Puberty
- Tall initially but short adult height due to early epiphyseal closure
C. Genetic Syndromes
Marfan Syndrome
- Tall, long limbs
- Arm span > height
- Lens dislocation
- Aortic dilation
Klinefelter Syndrome (XXY)
- Tall males
- Small testes, infertility
Sotos Syndrome
- Cerebral gigantism
- Developmental delay
11. Evaluation of Tall Stature
- Growth velocity trend
- Bone age
- Puberty status
- Dysmorphic features
- IGF-1 level if GH excess suspected
12. Management of Tall Stature
- Reassurance in familial cases
- Treat endocrine disorders:
* GH tumor surgery/medical therapy
* Antithyroid drugs
- Precocious puberty: GnRH analogs
13. Red Flags (Urgent Referral)
- Growth velocity falling rapidly
- Height crossing percentiles downward
- Dysmorphism
- Delayed or absent puberty
- Neurologic symptoms (headache, vision changes)
Summary Table
| Condition | Bone Age | Growth Velocity | Key Feature |
| ---------------------- | ----------------------- | --------------- | ---------------- |
| Familial short stature | Normal | Normal | Short parents |
| CDGP | Delayed | Normal | Late puberty |
| GH deficiency | Delayed | Low | Increased fat |
| Hypothyroidism | Delayed | Low | Weight gain |
| Chronic disease | Normal/slightly delayed | Low | Poor weight gain |
| Familial tall stature | Normal | Normal | Tall parents |
| GH excess | Advanced | High | Coarse features |
| Marfan | Normal | Normal/high | Long limbs |