Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
This article is being expanded for more depth. Check back soon!
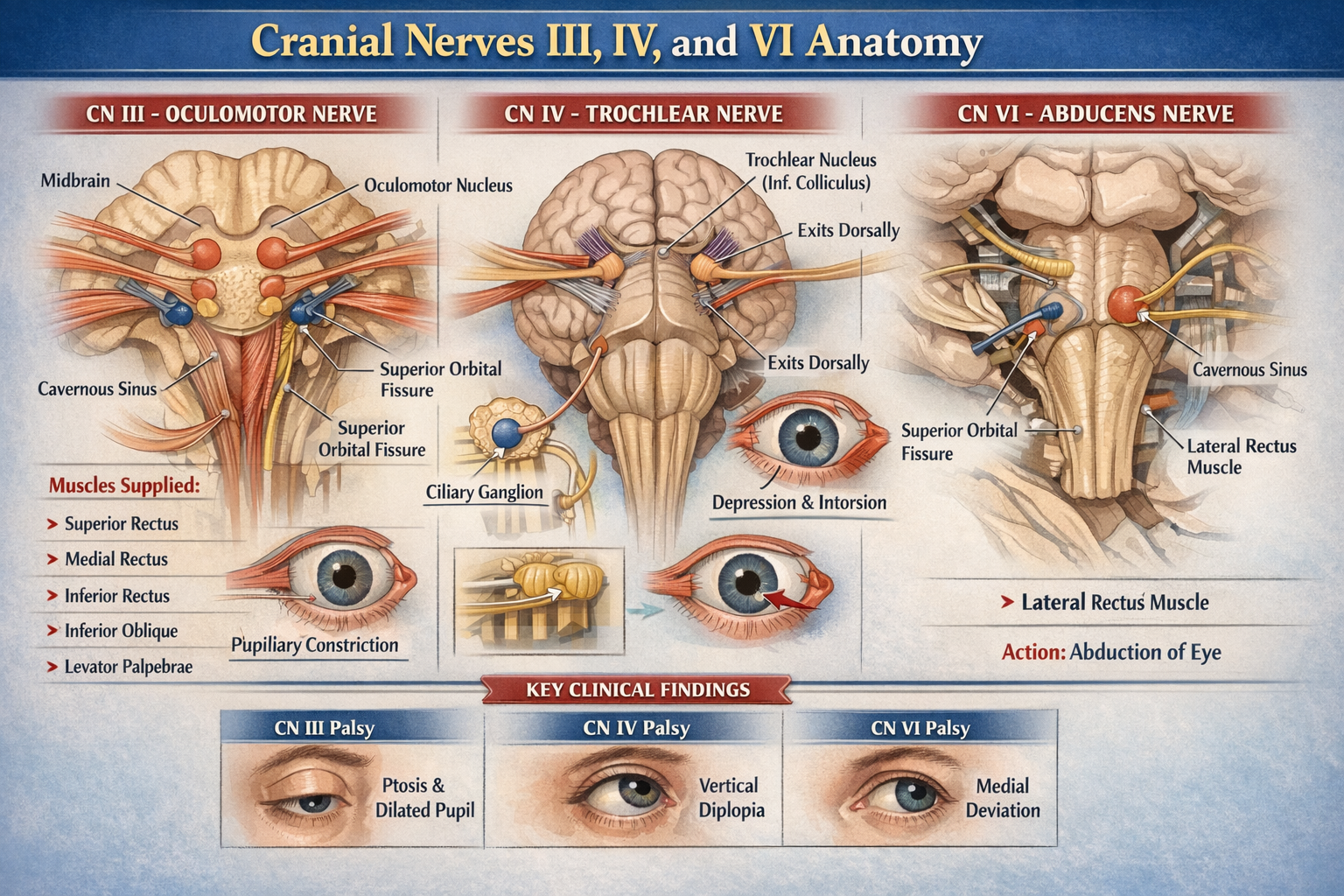
Cranial Nerves III IV VI Anatomy Detailed Overview for Medical Students
Frequently Asked Questions
What are cranial nerves III IV and VI?
Cranial nerves III IV and VI are motor cranial nerves responsible for controlling eye movements. They innervate the extraocular muscles that move the eyeball and maintain visual alignment.
What is the main function of the oculomotor nerve?
The oculomotor nerve supplies most extraocular muscles, elevates the upper eyelid, constricts the pupil, and enables accommodation of the lens.
Where is the oculomotor nerve nucleus located?
The oculomotor nuclear complex is located in the midbrain at the level of the superior colliculus.
Which muscles are supplied by cranial nerve III?
Cranial nerve III supplies superior rectus, inferior rectus, medial rectus, inferior oblique, and levator palpebrae superioris muscles.
What is unique about the trochlear nerve?
The trochlear nerve is the only cranial nerve that emerges from the dorsal surface of the brainstem, completely decussates, and has the longest intracranial course.
Which muscle is supplied by the trochlear nerve?
The trochlear nerve supplies the superior oblique muscle.
What is the primary action of the superior oblique muscle?
The superior oblique muscle causes intorsion and depression of the eyeball, especially when the eye is adducted.
Where is the abducens nerve nucleus located?
The abducens nerve nucleus is located in the dorsal pons beneath the facial colliculus.
Which muscle is innervated by the abducens nerve?
The abducens nerve innervates the lateral rectus muscle.
What movement is produced by the lateral rectus muscle?
The lateral rectus muscle abducts the eyeball.
Which cranial nerves pass through the cavernous sinus?
Cranial nerves III IV and VI pass through the cavernous sinus, with cranial nerve VI lying closest to the internal carotid artery.
Through which opening do cranial nerves III IV and VI enter the orbit?
All three nerves enter the orbit through the superior orbital fissure.
Why is the abducens nerve commonly affected in raised intracranial pressure?
The abducens nerve has a long intracranial course and a sharp bend over the petrous apex, making it vulnerable to stretching in raised intracranial pressure.
What are the features of oculomotor nerve palsy?
Oculomotor nerve palsy causes ptosis, dilated pupil, loss of accommodation, and deviation of the eye downward and outward.
What clinical symptom is typical of trochlear nerve palsy?
Trochlear nerve palsy typically presents with vertical diplopia that worsens when looking downwards, such as while descending stairs.
What eye position is seen in abducens nerve palsy?
Abducens nerve palsy causes medial deviation of the eye due to unopposed action of the medial rectus muscle.
Which parasympathetic fibers travel with the oculomotor nerve?
Parasympathetic fibers from the Edinger–Westphal nucleus travel with the oculomotor nerve to the ciliary ganglion.
What is the function of the ciliary ganglion?
The ciliary ganglion provides parasympathetic innervation to the sphincter pupillae and ciliary muscle.
Which cranial nerve enters the orbit outside the common tendinous ring?
The trochlear nerve enters the orbit outside the common tendinous ring.
Why are cranial nerves III IV and VI clinically important?
These nerves are essential for coordinated eye movements, binocular vision, and pupillary reflexes, and their lesions cause characteristic diplopia and eye deviation patterns.
MCQ Test - Cranial Nerves III IV VI Anatomy Detailed Overview for Medical Students
Progress:
0/0
Time: 00:00
No MCQs available for this article.