Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
Anatomy of Spinal Cord Complete Guide Location Structure Tracts Pathways
Frequently Asked Questions
What is the anatomical location of the spinal cord?
The spinal cord lies within the vertebral canal, extending from the foramen magnum above to the level of L1–L2 vertebrae in adults, where it ends as the conus medullaris.
What is the extent of the spinal cord in adults and newborns?
Adults: Foramen magnum to L1–L2 Newborns: Foramen magnum to L3–L4 The apparent ascent occurs due to differential growth of the vertebral column.
What are the modifications of pia mater in the spinal cord?
The pia mater is modified to form: Filum terminale Denticulate ligaments Linea splendens These structures stabilize and anchor the spinal cord within the vertebral canal.
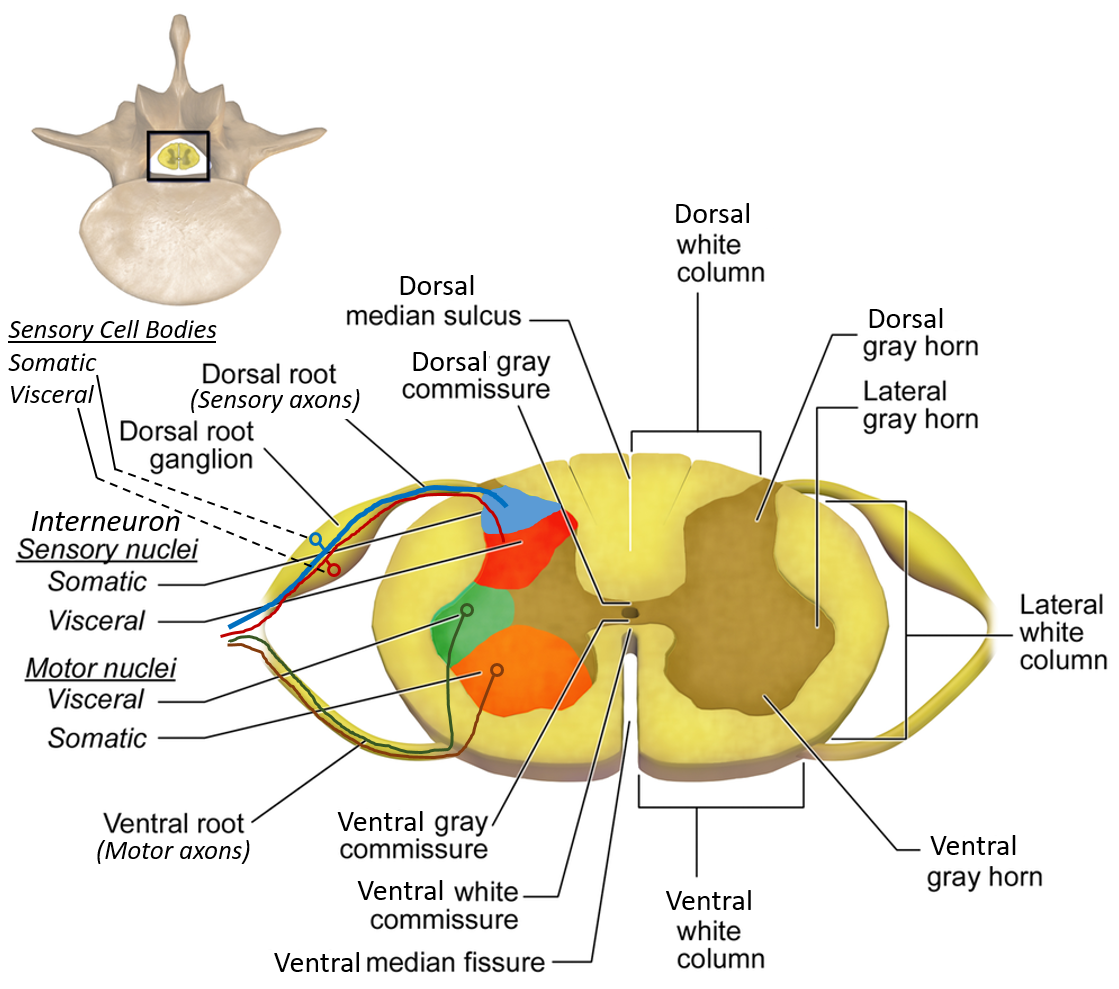
What are the horns of grey matter in the spinal cord?
The grey matter is divided into: Anterior horn: Motor neurons Posterior horn: Sensory neurons Lateral horn: Autonomic neurons (T1–L2, S2–S4)
Which neurons are found in the anterior horn?
The anterior horn contains lower motor neurons, including: Alpha motor neurons (extrafusal muscle fibers) Gamma motor neurons (muscle spindle regulation)
What nuclei are present in the posterior horn?
Important posterior horn nuclei include: Substantia gelatinosa (pain modulation) Nucleus proprius (touch and pressure) Clarke’s column (unconscious proprioception)
What is the difference between UMN and LMN?
UMN lesion: Spastic paralysis, hyperreflexia, Babinski sign LMN lesion: Flaccid paralysis, muscle wasting, fasciculations
What is the function of the anterior spinothalamic tract?
The anterior spinothalamic tract carries crude touch and pressure sensations.
MCQ Test - Anatomy of Spinal Cord Complete Guide Location Structure Tracts Pathways
Progress:
0/0
Time: 00:00
No MCQs available for this article.