Neonatal Resuscitation (NRP) – Full Detailed Guide
1. Definition
Neonatal resuscitation is the set of emergency interventions provided to a newborn immediately after birth to establish:
- Effective breathing
- Adequate heart rate
- Proper oxygenation and circulation
Most babies transition normally, but ~10% need assistance, and ~1% require extensive resuscitation.
2. Physiology of Birth Transition
At birth, the newborn must rapidly shift from placental to lung-based oxygenation:
Key changes:
- Lung fluid clears
- First breaths expand alveoli
- Pulmonary vascular resistance drops
- Blood flow increases through lungs
- Closure of fetal shunts (ductus arteriosus, foramen ovale)
Failure → asphyxia, bradycardia, hypoxia
3. Causes / Risk Factors
Maternal factors:
- Diabetes
- Hypertension
- Infection (chorioamnionitis)
- Prolonged labor
Fetal factors:
- Prematurity
- Growth restriction
- Congenital anomalies
Intrapartum factors:
- Meconium-stained liquor
- Cord prolapse
- Placental abruption
- Shoulder dystocia
4. Preparation Before Delivery
Resuscitation team readiness:
- At least 1 trained person for every delivery
- Extra skilled staff if high-risk birth
Equipment checklist:
- Radiant warmer
- Suction device
- Bag-mask ventilator
- Oxygen blender
- Pulse oximeter
- Endotracheal tubes, laryngoscope
- Umbilical catheter supplies
- Emergency drugs (epinephrine)
5. Initial Rapid Assessment
Immediately after birth ask:
- Term gestation?
- Good muscle tone?
- Breathing or crying?
If YES to all → Routine care
If NO → Start resuscitation
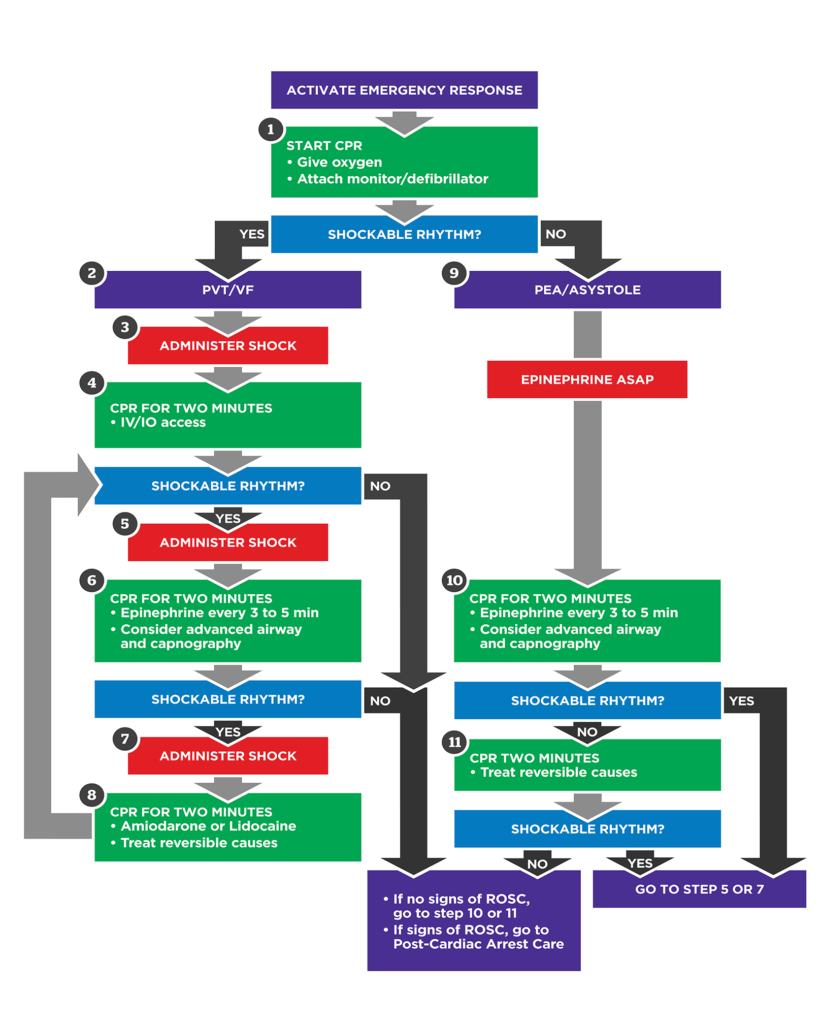
6. Neonatal Resuscitation Algorithm (Stepwise)
Step 1: Initial Stabilization (First 30 sec)
Actions (Warm, Dry, Stimulate):
- Provide warmth (prevent hypothermia)
- Position airway (sniffing position)
- Clear secretions only if obstructing
- Dry thoroughly
- Gentle stimulation
Evaluate:
- Respirations
- Heart rate (HR)
- Color / oxygen saturation
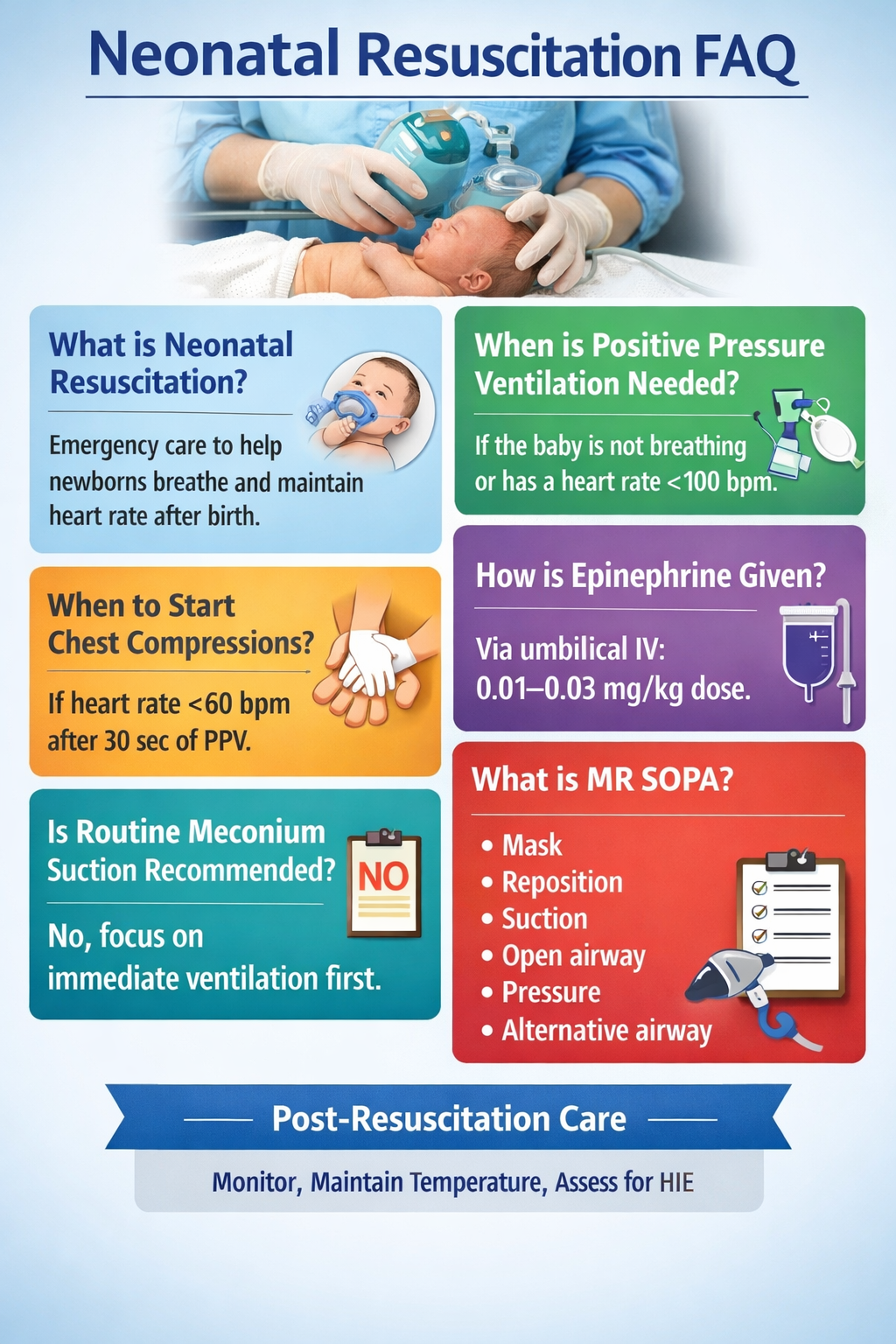
Step 2: Positive Pressure Ventilation (PPV)
Indications:
- Apnea or gasping
- HR < 100 bpm
Technique:
- Bag-mask ventilation
- Rate: 40–60 breaths/min
- Use room air initially in term babies
Oxygen:
- Term: start with 21%
- Preterm: start with 21–30%
Target SpO₂ rises gradually:
- 1 min: 60–65%
- 5 min: 80–85%
- 10 min: 85–95%
Ventilation Corrective Steps (MR SOPA)
If chest not rising:
- Mask adjustment
- Reposition airway
- Suction mouth/nose
- Open mouth
- Pressure increase
- Alternative airway (ET tube/LMA)
Step 3: Chest Compressions
Indication:
- HR < 60 bpm after 30 sec of effective PPV
Method:
- Two-thumb technique on lower sternum
Ratio:
- 3 compressions : 1 ventilation
- 90 compressions + 30 breaths = 120 events/min
Oxygen:
- Increase to 100% during compressions
Step 4: Medications
Indication:
- HR < 60 bpm despite ventilation + compressions
7. Drugs in Neonatal Resuscitation (Detailed)
Epinephrine (Adrenaline)
Indication:
- Severe bradycardia/asystole (HR < 60)
Mechanism:
- α1 vasoconstriction → improves coronary perfusion
- β1 stimulation → increases HR and contractility
Dose:
- IV/umbilical: 0.01–0.03 mg/kg
* (0.1–0.3 mL/kg of 1:10,000 solution)
- Endotracheal (less effective): 0.05–0.1 mg/kg
Pharmacokinetics:
- Rapid onset (seconds IV)
- Short half-life
Adverse effects:
- Tachycardia
- Hypertension
- Arrhythmias
Contraindications:
- None in cardiac arrest
Monitoring:
- HR response every 30 sec
Counselling:
- Emergency life-saving drug only
Volume Expansion (Normal Saline)
Indication:
- Suspected hypovolemia (blood loss, shock)
- Poor perfusion, weak pulses
Dose:
- 10 mL/kg IV over 5–10 min
Adverse effects:
- Fluid overload
- Pulmonary edema
Glucose
Indication:
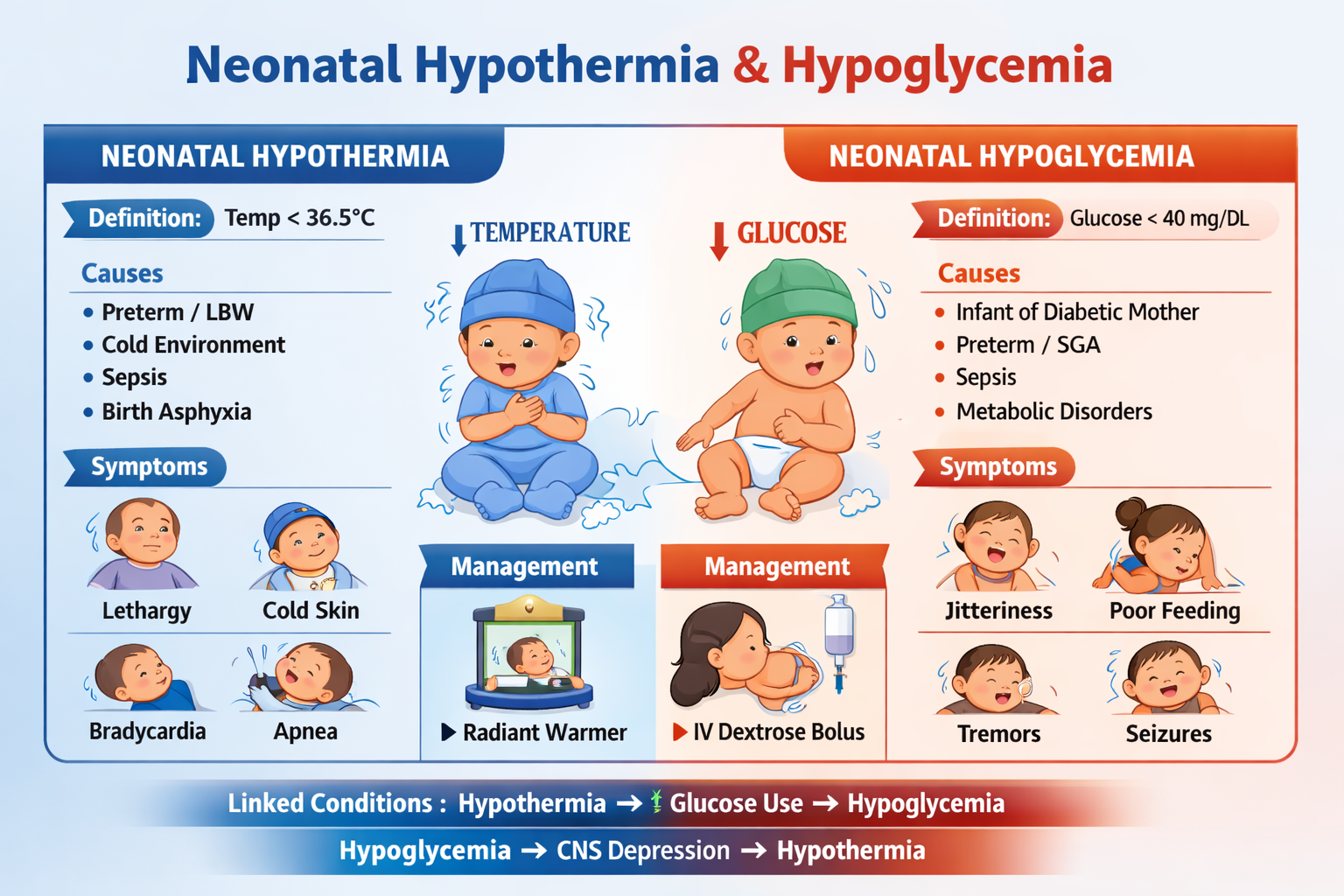
- Prolonged resuscitation → hypoglycemia risk
Dose:
- D10W bolus 2 mL/kg IV
Naloxone (Rarely Used Now)
Not recommended routinely due to withdrawal risk.
8. Airway Management
Endotracheal Intubation Indications:
- Prolonged PPV
- Need for suction below cords
- Chest compressions
- Suspected diaphragmatic hernia
Tube size:
- <1 kg: 2.5 mm
- 1–2 kg: 3.0 mm
- > 2 kg: 3.5 mm
9. Special Situations
Meconium-Stained Liquor
- No routine suctioning
- If non-vigorous + obstruction suspected → intubation suction
Premature Infant
- Prevent heat loss (plastic wrap)
- Gentle ventilation (avoid lung injury)
- CPAP may help
Congenital Diaphragmatic Hernia
- Avoid bag-mask ventilation
- Immediate intubation
10. Post-Resuscitation Care
After stabilization:
- NICU admission
- Maintain temperature (36.5–37.5°C)
- Monitor glucose, electrolytes
- Continuous oxygen saturation + ECG
- Treat seizures if present
- Consider therapeutic hypothermia if HIE suspected
11. Complications
- Hypoxic ischemic encephalopathy (HIE)
- Pneumothorax
- Pulmonary hemorrhage
- Intracranial hemorrhage (preterm)
- Long-term neurodevelopmental delay
12. Key Take-Home Points
- Ventilation is the most important step
- Most newborns respond to PPV alone
- Chest compressions only if HR < 60
- Epinephrine is last step after effective ventilation