✅ NEONATAL HYPOTHERMIA
1. Definition
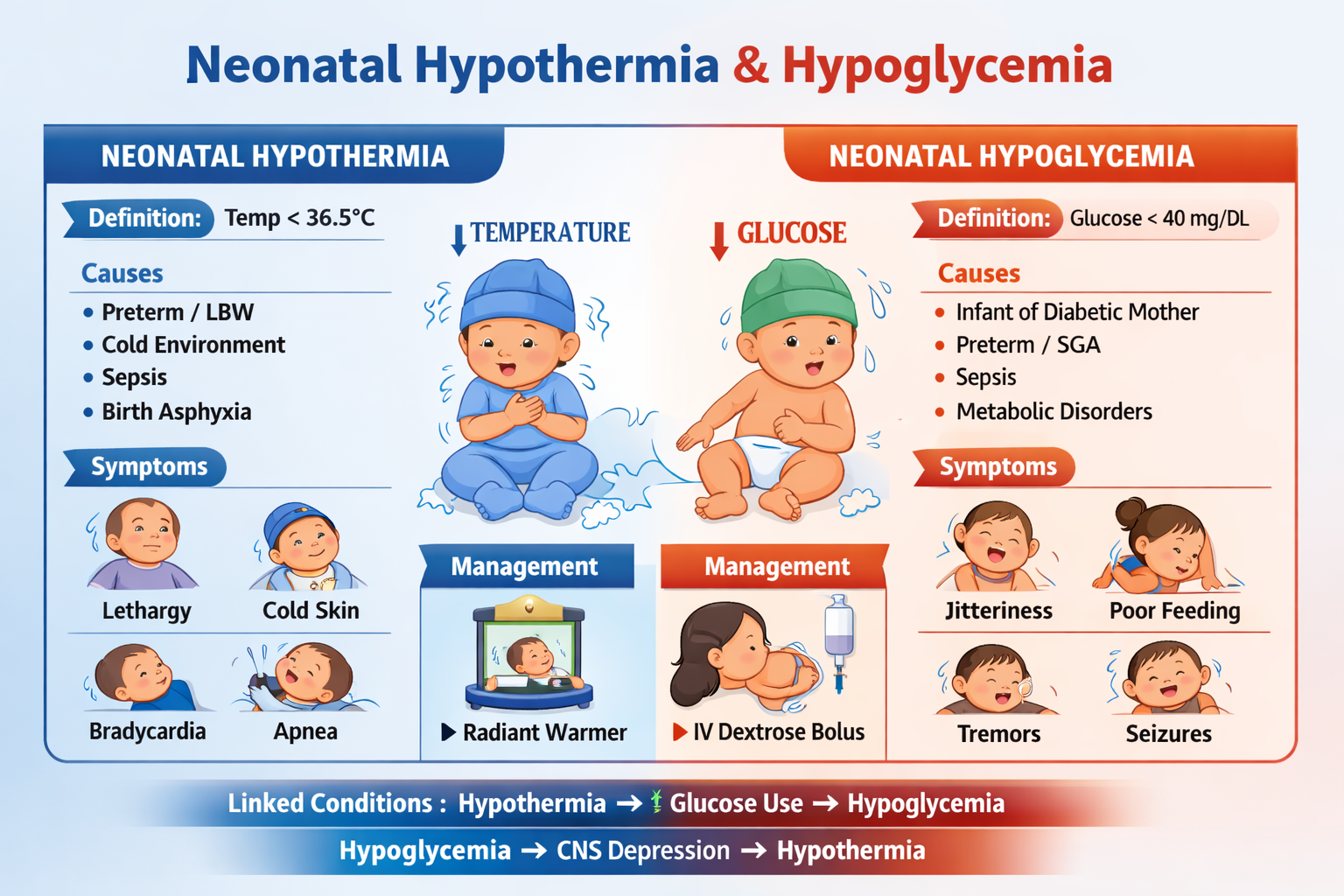
Neonatal hypothermia is a condition where a newborn’s core body temperature falls below normal due to poor thermoregulation.
- Normal neonatal temperature: 36.5–37.5°C
- Hypothermia: < 36.5°C
WHO Classification
| Severity | Temperature |
| ------------------ | ----------- |
| Mild (Cold stress) | 36.0–36.4°C |
| Moderate | 32.0–35.9°C |
| Severe | < 32°C |
2. Pathophysiology
Newborns are highly prone to hypothermia because of:
- Large surface area to body weight ratio
- Thin skin + minimal subcutaneous fat
- Poor shivering response
- Heat loss through evaporation, convection, conduction, radiation
- Reliance on brown fat metabolism (non-shivering thermogenesis)
Consequences
Hypothermia leads to:
- Increased oxygen consumption
- Hypoglycemia
- Metabolic acidosis
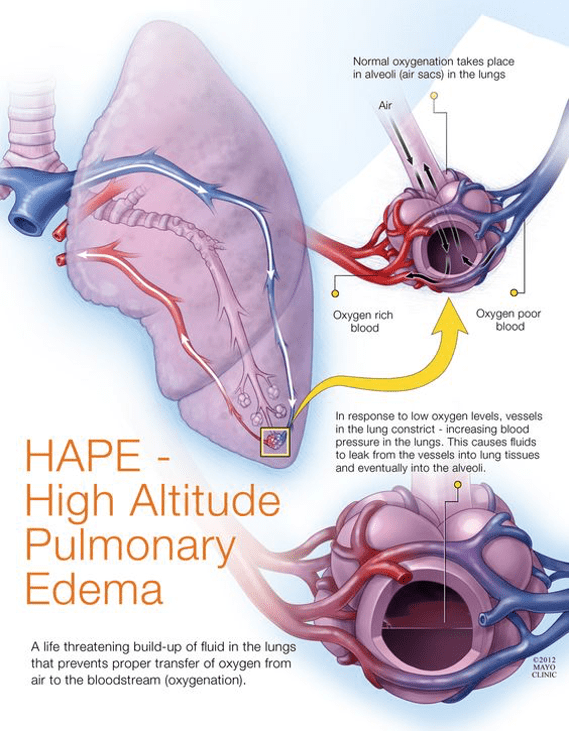
- Pulmonary vasoconstriction → PPHN
- Sepsis risk increases
3. Causes / Risk Factors
Environmental
- Cold delivery room
- Wet baby not dried
- Delayed wrapping
- Poor incubator warming
Neonatal Factors
- Prematurity
- Low birth weight
- IUGR
- Birth asphyxia
Pathological Causes
- Neonatal sepsis
- CNS depression
- Hypoglycemia
4. Clinical Features
Mild Hypothermia (Cold stress)
- Cool extremities
- Peripheral cyanosis
- Irritability
- Tachypnea
Moderate to Severe
- Lethargy
- Poor feeding
- Weak cry
- Bradycardia
- Hypotonia
- Apnea
- Hypoglycemia
- Metabolic acidosis
5. Diagnosis / Investigations
Temperature Monitoring
- Axillary digital thermometer preferred
Labs (if moderate/severe)
- Blood glucose
- Blood gas (metabolic acidosis)
- CBC + CRP
- Blood culture (rule out sepsis)
6. Differential Diagnosis
- Neonatal sepsis
- Hypoglycemia
- Birth asphyxia
- Congenital hypothyroidism
- CNS depression (drug exposure)
7. Management (Stepwise)
A. Immediate Stabilization
- Dry baby thoroughly
- Remove wet linen
- Warm room temperature (≥ 26°C)
B. Rewarming
Mild Hypothermia
- Skin-to-skin (Kangaroo mother care)
- Warm blankets
- Breastfeeding encouraged
Moderate Hypothermia
- Radiant warmer or incubator
- Monitor vitals every 15–30 min
Severe Hypothermia
- NICU care
- Slow controlled rewarming
- IV fluids + glucose
- Treat underlying cause (sepsis)
C. Treat Complications
- Hypoglycemia correction
- Oxygen support if respiratory distress
- Antibiotics if sepsis suspected
8. Prevention
- Warm chain at birth
- Immediate drying
- Early breastfeeding
- Kangaroo care
- Avoid exposure during transport
✅ NEONATAL HYPOGLYCEMIA
1. Definition
Neonatal hypoglycemia is defined as low plasma glucose levels causing risk of brain injury.
Operational Thresholds
| Age | Plasma Glucose Concern |
| ------------ | ---------------------- |
| First 4 hrs | < 25 mg/dL |
| 4–24 hrs | < 35 mg/dL |
| After 24 hrs | < 45 mg/dL |
2. Pathophysiology
At birth, placental glucose supply stops → newborn must maintain glucose by:
- Glycogenolysis
- Gluconeogenesis
- Ketogenesis
Hypoglycemia occurs when:
- Glycogen stores are low
- Insulin is high
- Feeding is delayed
- Metabolic disorders exist
Brain Risk
Prolonged hypoglycemia → seizures → permanent neurodevelopmental impairment.
3. Causes / Risk Factors
Increased Insulin (Hyperinsulinism)
- Infant of diabetic mother (IDM)
- Congenital hyperinsulinism
Low Stores
- Prematurity
- IUGR / SGA
- Malnutrition
Increased Demand
- Sepsis
- Hypothermia
- Asphyxia
Inborn Errors
- Galactosemia
- Fatty acid oxidation defects
- Adrenal insufficiency
4. Clinical Features
Often Asymptomatic (early)
Symptomatic Signs
- Jitteriness
- Tremors
- High-pitched cry
- Poor feeding
- Lethargy
- Apnea
- Hypotonia
- Cyanosis
- Seizures (late sign)
5. Diagnosis / Investigations
Bedside Screening
- Glucometer (capillary)
Confirmatory Test
- Plasma glucose (lab)
Additional Workup (recurrent/severe)
- Serum insulin
- Cortisol
- Growth hormone
- Ketones
- Lactate
- Metabolic screen
6. Differential Diagnosis
- Hypocalcemia
- Neonatal seizures
- Sepsis
- Drug withdrawal
- Intracranial hemorrhage
7. Management (Stepwise)
A. Asymptomatic Hypoglycemia
Glucose 25–45 mg/dL
- Early feeding (breastmilk/formula)
- Recheck glucose in 30 min
If persistent
- Start IV glucose
B. Symptomatic or Severe Hypoglycemia
Immediate Bolus
10% dextrose 2 mL/kg IV
Continuous Infusion
Start 10% dextrose infusion
- GIR: 4–6 mg/kg/min initially
- Increase up to 8–12 mg/kg/min if needed
C. If Refractory
- Consider hyperinsulinism
- Add:
Glucagon
0.1 mg/kg IM/IV
Diazoxide (for hyperinsulinism)
8. Drug Details
✅ Dextrose (10%)
Indication
- Acute neonatal hypoglycemia
Mechanism
- Provides immediate glucose substrate
Dose
- Bolus: 2 mL/kg IV
- Infusion: Adjust GIR
Adverse Effects
- Hyperglycemia
- Fluid overload
- Extravasation injury
Monitoring
- Glucose every 30–60 min
- Electrolytes
Counseling
- Early feeding prevents recurrence
✅ Glucagon
Indication
- Hypoglycemia due to hyperinsulinism
Mechanism
- Stimulates glycogenolysis
Dose
- 0.1 mg/kg IM/IV
Adverse Effects
- Vomiting
- Tachycardia
Contraindication
- No glycogen stores (severe malnutrition)
9. Prevention
- Early breastfeeding within 1 hour
- Screen high-risk babies:
* IDM
* Preterm
* SGA/LGA
- Maintain warmth (prevent hypothermia)
🔥 Key Link Between Both Conditions
Hypothermia → Increased glucose use → Hypoglycemia
Hypoglycemia → CNS depression → Poor thermoregulation → Hypothermia
They often occur together and must be treated simultaneously.