Neonatal Jaundice (Paediatrics)
1. Definition
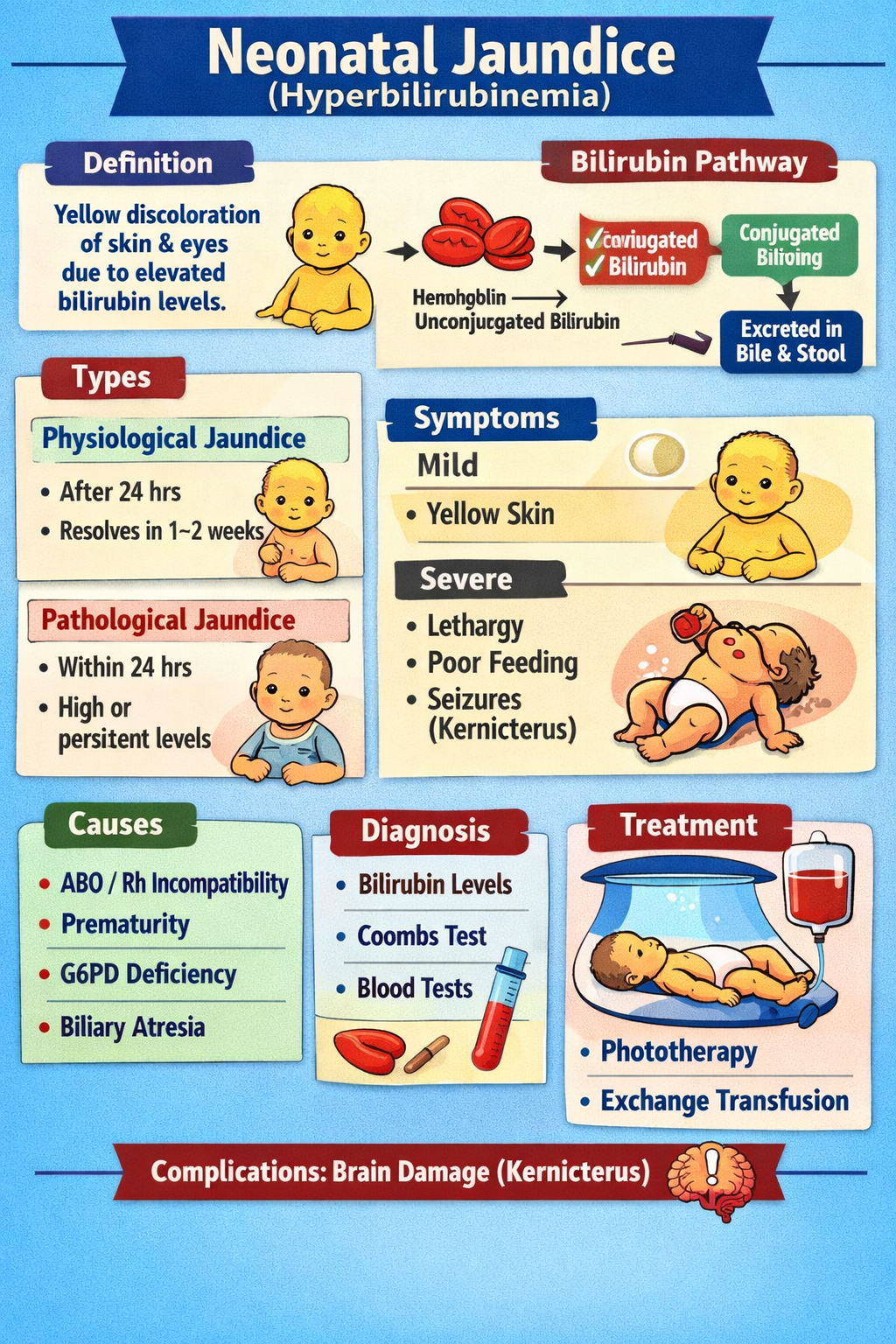
Neonatal jaundice is the yellow discoloration of skin, sclera, and mucous membranes in newborn infants caused by elevated serum bilirubin levels (hyperbilirubinemia) during the neonatal period (first 28 days of life).
- Clinically visible when total serum bilirubin (TSB) > 5 mg/dL.
- Occurs in about 60% of term neonates and 80% of preterm neonates.
2. Bilirubin Metabolism (Pathophysiology)
Normal Bilirubin Pathway
- Hemoglobin breakdown
* RBC destruction → heme → biliverdin → unconjugated bilirubin
- Transport
* Unconjugated bilirubin binds albumin in plasma.
- Hepatic uptake
* Liver cells take bilirubin.
- Conjugation
* Enzyme UDP-glucuronyl transferase converts unconjugated → conjugated bilirubin.
- Excretion
* Conjugated bilirubin → bile → intestine → stool.
Why Neonates Develop Jaundice
Neonates have several physiological factors:
- Increased bilirubin production
* Higher RBC mass
* Short RBC lifespan (70–90 days)
- Immature liver
* Reduced UDP-glucuronyl transferase activity
- Increased enterohepatic circulation
* Gut converts conjugated bilirubin back to unconjugated bilirubin.
3. Types of Neonatal Jaundice
1. Physiological Jaundice
Most common.
Features
| Feature | Description |
| ----------------- | --------------------------------- |
| Onset | After 24 hours of life |
| Peak | Day 3–5 (term), Day 5–7 (preterm) |
| Maximum bilirubin | <12 mg/dL (term) |
| Duration | <7 days (term) |
Mechanism
- Increased bilirubin production
- Immature liver conjugation
2. Pathological Jaundice
Criteria
Any of the following:
- Jaundice within first 24 hours
- Bilirubin rise >5 mg/dL/day
- Total bilirubin >15 mg/dL
- Direct bilirubin >2 mg/dL
- Jaundice lasting >14 days (term)
4. Causes of Neonatal Jaundice
A. Unconjugated Hyperbilirubinemia
Hemolytic Causes
- ABO incompatibility
- Rh incompatibility
- G6PD deficiency
- Hereditary spherocytosis
Non-Hemolytic Causes
- Physiological jaundice
- Prematurity
- Birth trauma (cephalohematoma)
- Polycythemia
- Sepsis
- Hypothyroidism
Breastfeeding Related
Breastfeeding jaundice
- Due to poor feeding → dehydration.
Breast milk jaundice
- Appears day 4–7
- Peaks at 2 weeks
B. Conjugated Hyperbilirubinemia (Cholestatic Jaundice)
Causes include:
- Biliary atresia
- Neonatal hepatitis
- Metabolic diseases
- Sepsis
- Galactosemia
- Alpha-1 antitrypsin deficiency
Direct bilirubin >2 mg/dL is abnormal.
5. Clinical Features
Skin Examination
Jaundice spreads head → toe (cephalocaudal progression).
Kramer scale
| Zone | Bilirubin level |
| --------------- | --------------- |
| Head and neck | ~5 mg/dL |
| Upper trunk | ~10 mg/dL |
| Lower trunk | ~12 mg/dL |
| Arms and thighs | ~15 mg/dL |
| Palms and soles | >20 mg/dL |
Symptoms
Most infants are asymptomatic.
Severe jaundice may cause:
- Poor feeding
- Lethargy
- Hypotonia
- High-pitched cry
6. Kernicterus (Bilirubin Encephalopathy)
Severe unconjugated bilirubin crosses blood-brain barrier.
Risk Factors
- Prematurity
- Hemolysis
- Sepsis
- Acidosis
- Hypoxia
- Low albumin
Clinical Stages
Early
- Lethargy
- Poor feeding
- Hypotonia
Intermediate
- Hypertonia
- Opisthotonus
- High-pitched cry
Advanced
- Seizures
- Coma
- Death
Long Term Complications
- Cerebral palsy
- Hearing loss
- Intellectual disability
- Dental enamel dysplasia
7. Investigations
Basic Tests
- Total serum bilirubin (TSB)
- Direct and indirect bilirubin
- Blood group (mother and baby)
- Direct Coombs test
- Complete blood count
- Peripheral smear
- Reticulocyte count
Additional Tests (If needed)
- G6PD assay
- Thyroid function test
- Liver function test
- Blood culture (if sepsis suspected)
- Ultrasound abdomen (for biliary atresia)
8. Management
Treatment depends on age in hours, gestational age, and bilirubin level.
1. Phototherapy
Mechanism
Blue light converts bilirubin into water-soluble photoisomers that can be excreted without conjugation.
Light wavelength
460–490 nm (blue light)
Indications
Based on bilirubin charts (AAP nomogram).
Approximate levels in term infant
| Age | Start Phototherapy |
| ------ | ------------------ |
| 24 hrs | ≥12 mg/dL |
| 48 hrs | ≥15 mg/dL |
| 72 hrs | ≥18 mg/dL |
Procedure
- Baby undressed
- Eyes covered
- Maintain hydration
- Turn infant regularly
Adverse Effects
- Dehydration
- Loose stools
- Skin rash
- Hyperthermia
- Bronze baby syndrome
2. Exchange Transfusion
Used when phototherapy fails.
Indications
- Bilirubin approaching 20–25 mg/dL
- Severe hemolysis
- Signs of kernicterus
Mechanism
- Removes bilirubin
- Removes maternal antibodies
- Replaces sensitized RBCs
Complications
- Electrolyte imbalance
- Infection
- Thrombocytopenia
- Hypoglycemia
3. Pharmacological Treatment
Phenobarbital
Indication
Enhances bilirubin conjugation.
Mechanism
Induces UDP-glucuronyl transferase enzyme.
Dose
5 mg/kg/day
Pharmacokinetics
- Long half-life
- Hepatic metabolism
Adverse Effects
- Sedation
- Respiratory depression
Contraindications
- Severe respiratory depression
Intravenous Immunoglobulin (IVIG)
Indication
Used in Rh or ABO hemolytic disease.
Mechanism
Reduces hemolysis by blocking Fc receptors.
Dose
0.5–1 g/kg IV
Adverse Effects
- Fever
- Hypotension
- Allergic reaction
9. Non-Pharmacological Measures
- Early initiation of breastfeeding
- Frequent feeding (8–12 times/day)
- Adequate hydration
- Monitor urine and stool output
10. Monitoring
During treatment monitor:
- Serum bilirubin levels
- Temperature
- Hydration status
- Weight
- Signs of kernicterus
11. Prevention
- Blood group screening in pregnancy
- Anti-D immunoglobulin for Rh negative mothers
- Early breastfeeding
- Early bilirubin screening
12. Prognosis
- Most cases resolve without complications.
- Early detection and treatment prevent kernicterus.
If you want, I can also give 30 MCQs on Neonatal Jaundice for NEET-PG, NEXT, and FMGE preparation.