MALNUTRITION IN PAEDIATRICS (DETAIL)
1. Definition
Malnutrition is a pathological state resulting from deficiency, excess, or imbalance of energy, protein, and other nutrients that adversely affects growth, development, and health.
In children, malnutrition mainly refers to:
- Undernutrition
- Protein–Energy Malnutrition (PEM)
- Micronutrient deficiencies
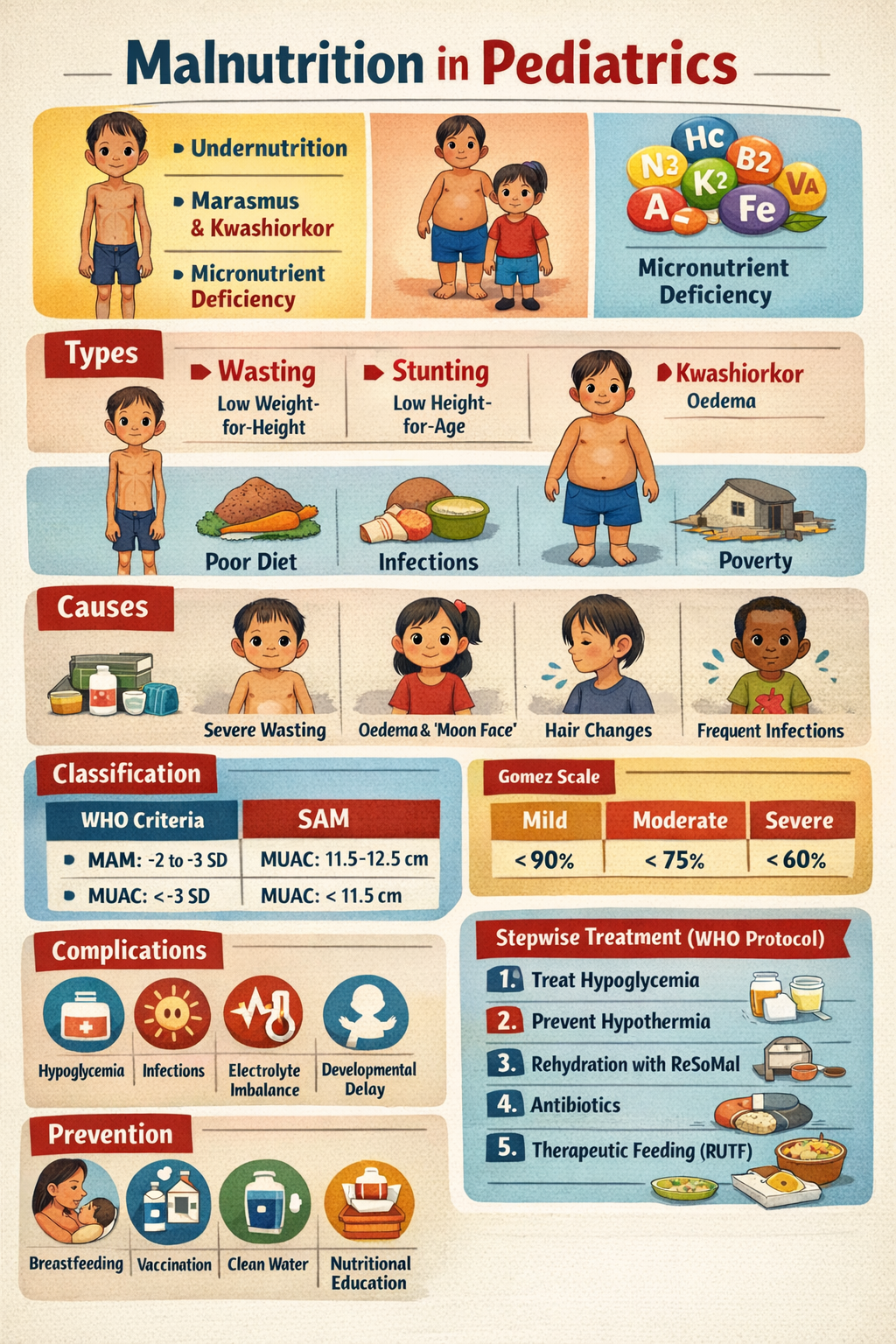
2. Types of Malnutrition
A. Undernutrition
Includes:
- Wasting → low weight-for-height (acute malnutrition)
- Stunting → low height-for-age (chronic malnutrition)
- Underweight → low weight-for-age
- Micronutrient deficiencies
B. Protein–Energy Malnutrition (PEM)
1. Marasmus
- Severe calorie deficiency
- Marked wasting
- No oedema
2. Kwashiorkor
- Protein deficiency with adequate calories
- Oedema present
3. Marasmic Kwashiorkor
- Combination of wasting + oedema
C. Overnutrition
- Childhood obesity (excess calories)
3. Etiology / Causes
Immediate Causes
- Inadequate dietary intake
- Recurrent infections (diarrhoea, pneumonia, TB)
Underlying Causes
- Poverty
- Food insecurity
- Poor breastfeeding practices
- Improper complementary feeding
- Poor sanitation
- Lack of maternal education
Medical Causes
- Malabsorption syndromes (celiac disease)
- Congenital heart disease
- Chronic kidney/liver disease
- HIV infection
- Cancer
4. Pathophysiology
Energy Deficiency
- Body uses fat stores → weight loss
- Muscle protein breakdown → wasting
- Impaired immunity
Protein Deficiency
- Reduced albumin → oedema
- Fatty liver infiltration
- Impaired wound healing
Micronutrient Deficiency
- Iron → anaemia
- Vitamin A → blindness
- Zinc → impaired immunity and growth failure
5. Clinical Features
A. General Features
- Failure to thrive
- Weight loss or poor weight gain
- Irritability or lethargy
- Delayed milestones
- Frequent infections
B. Marasmus
- Severe wasting (“skin and bones”)
- Loss of subcutaneous fat
- Old-man face
- No oedema
- Alert but hungry
C. Kwashiorkor
- Bilateral pitting oedema
- Moon face
- Flaky paint dermatosis
- Hair changes (sparse, hypopigmented)
- Hepatomegaly (fatty liver)
- Apathy, poor appetite
D. Severe Acute Malnutrition (SAM) Signs
- Weight-for-height < –3 SD
- MUAC < 11.5 cm
- Bilateral oedema
- Visible severe wasting
6. Classification
WHO Classification of Acute Malnutrition
| Category | Criteria |
| -------- | --------------------------------------- |
| MAM | WHZ –2 to –3 SD OR MUAC 11.5–12.5 cm |
| SAM | WHZ < –3 SD OR MUAC < 11.5 cm OR oedema |
Gomez Classification (Weight for Age)
| Grade | % of Expected Weight |
| -------- | -------------------- |
| Mild | 75–89% |
| Moderate | 60–74% |
| Severe | <60% |
7. Investigations
Basic Tests
- CBC → anaemia, infection
- Serum electrolytes
- Blood glucose (hypoglycaemia)
- Serum albumin (low in kwashiorkor)
Micronutrient Levels
- Iron studies
- Vitamin D, B12 (if suspected)
Identify Cause
- Stool examination (parasites)
- Celiac screen (tTG-IgA)
- HIV testing if indicated
- TB screening
8. Complications
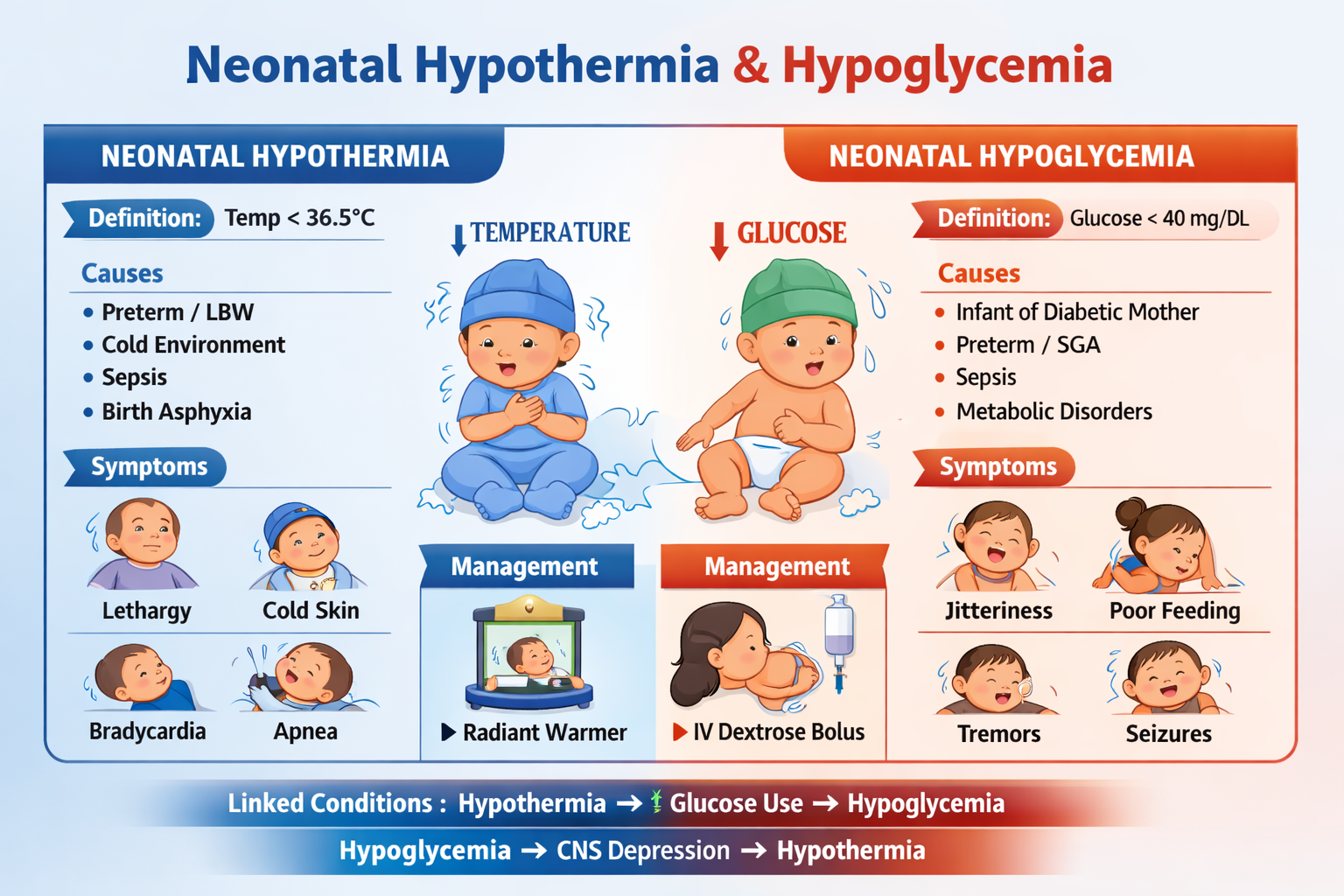
- Hypoglycaemia
- Hypothermia
- Severe infections/sepsis
- Electrolyte imbalance (low K+, Mg++)
- Heart failure during refeeding
- Developmental delay
- High mortality
9. Management (Stepwise WHO Protocol)
Emergency Phase (First 1–7 days)
Step 1: Treat Hypoglycaemia
- If glucose <54 mg/dL:
* 10% dextrose 5 ml/kg IV
* Start feeding immediately
Step 2: Prevent Hypothermia
- Keep child warm
- Skin-to-skin contact
- Warm feeds
Step 3: Treat Dehydration Carefully
Use ReSoMal (not ORS standard)
- 5–10 ml/kg every 30 min for 2 hours
- Avoid IV fluids unless shock
Step 4: Treat Infections (Empirical Antibiotics)
Ampicillin + Gentamicin
- Ampicillin: 50 mg/kg IV/IM every 6 hr
- Gentamicin: 7.5 mg/kg once daily
If oral:
- Amoxicillin: 30 mg/kg/day in 2 doses
Step 5: Correct Micronutrient Deficiency
- Vitamin A
- Multivitamins
- Zinc
- Folic acid
⚠ Iron delayed until stabilization.
Step 6: Start Therapeutic Feeding (F-75 Formula)
- Low protein, low sodium starter feed
- Prevent refeeding syndrome
Rehabilitation Phase
Step 7: Catch-Up Growth (F-100 or RUTF)
- Ready-to-use therapeutic food (RUTF)
- High calorie diet: 150–220 kcal/kg/day
Step 8: Iron Supplementation (after 1 week)
- Elemental iron: 3 mg/kg/day
Step 9: Sensory Stimulation & Emotional Support
- Play therapy
- Mother–child bonding
Step 10: Prepare for Follow-Up
- Nutrition counselling
- Growth monitoring
- Immunization completion
10. Drugs in Detail
Vitamin A
Indication
- Prevent blindness, improve immunity
Dose (WHO)
- <6 months: 50,000 IU
- 6–12 months: 100,000 IU
- > 12 months: 200,000 IU
Adverse effects
- Bulging fontanelle (rare overdose)
Folic Acid
Dose
- 5 mg once, then 1 mg/day
Role
- Prevent megaloblastic anaemia
Zinc
Dose
- 2 mg/kg/day
Benefits
- Improves immunity and gut recovery
Iron
Dose
- 3 mg/kg/day elemental iron
Start
- Only after stabilization (day 7+)
Side effects
- GI upset, constipation
Antibiotics
Ampicillin
- 50 mg/kg IV q6h
Gentamicin
- 7.5 mg/kg OD
Monitoring
- Renal function, hearing toxicity
11. Prevention
Infant Feeding
- Exclusive breastfeeding for 6 months
- Complementary feeding after 6 months
Community Measures
- Safe water, sanitation
- Deworming
- Vitamin A prophylaxis
- Growth monitoring programs
Immunization
- Prevent infection-related malnutrition
12. Prognosis
Depends on:
- Early recognition
- Presence of complications
- Quality of rehabilitation
- Underlying disease treatment
With proper WHO protocol, survival improves significantly.