Neonatal Jaundice (Hyperbilirubinemia) — Complete Detail
1. Definition
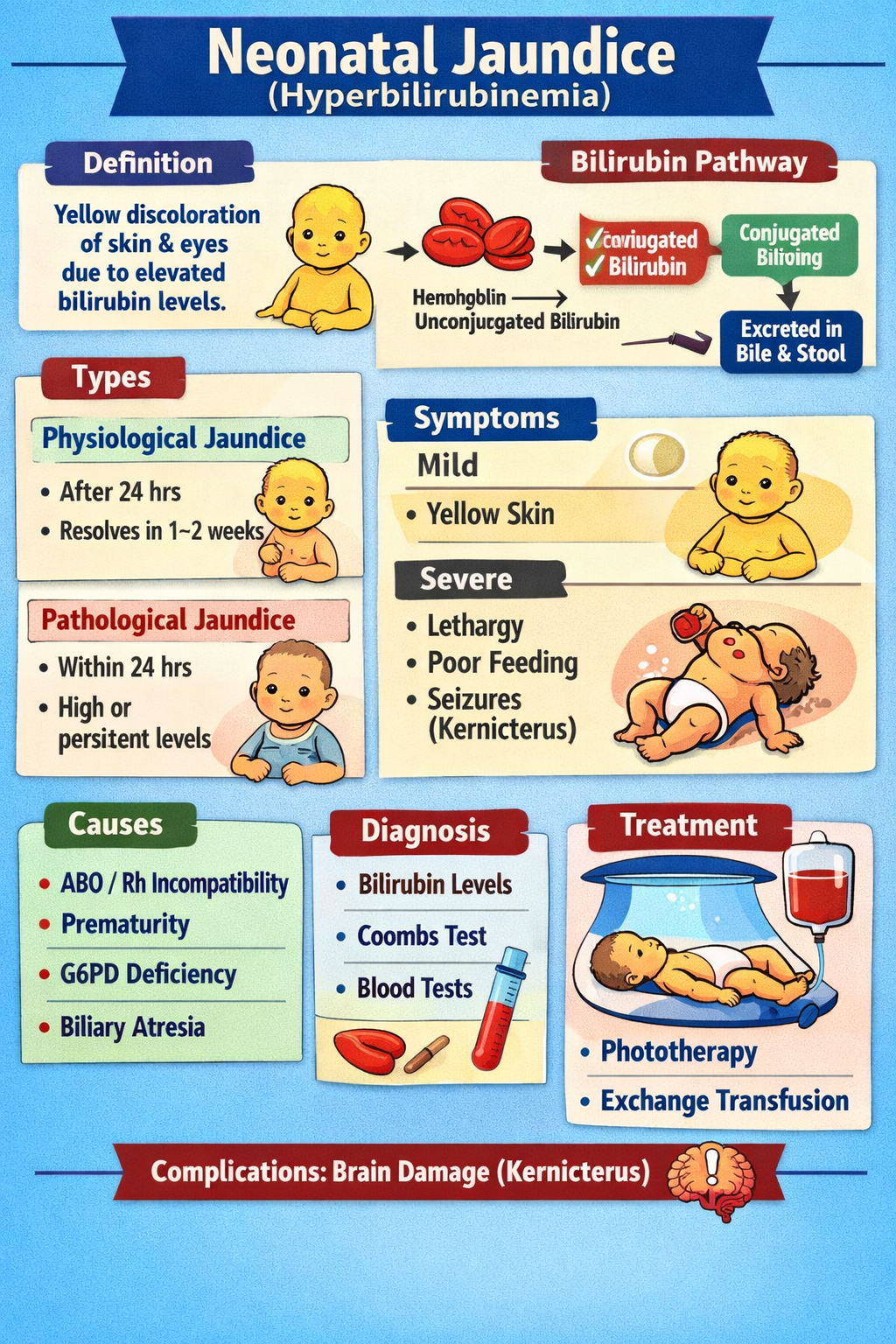
Neonatal jaundice is the yellow discoloration of the skin and sclera in newborns caused by elevated serum bilirubin levels.
- Visible jaundice usually appears when:
* Total serum bilirubin (TSB) > 5 mg/dL (85 µmol/L)
It is extremely common:
- ~60% of term babies
- ~80% of preterm babies
2. Pathophysiology
Bilirubin is produced from breakdown of red blood cells:
Stepwise mechanism:
- Hemoglobin breakdown → Unconjugated bilirubin
- Unconjugated bilirubin binds to albumin in blood
- Transported to liver
- Liver enzyme UDP-glucuronyl transferase conjugates bilirubin
- Conjugated bilirubin excreted into bile → intestine
- Some bilirubin is reabsorbed via enterohepatic circulation
Why newborns develop jaundice?
- Increased RBC turnover (shorter RBC lifespan)
- Immature liver conjugation enzymes
- Increased enterohepatic circulation
- Low feeding → delayed bilirubin excretion
3. Classification
A. Physiological Jaundice
Normal and benign.
- Appears after 24 hours
- Peaks:
* Term: day 3–5
* Preterm: day 5–7
- Resolves by 1–2 weeks
B. Pathological Jaundice
Suspect if:
- Jaundice within first 24 hours
- Rapid rise > 0.5 mg/dL/hour
- TSB > 95th percentile
- Conjugated bilirubin > 2 mg/dL
- Persists > 2 weeks (term)
4. Causes / Triggers
Unconjugated Hyperbilirubinemia
Increased production
- Hemolytic disease:
* ABO incompatibility
* Rh incompatibility
- G6PD deficiency
- Hereditary spherocytosis
- Cephalhematoma / bruising
- Polycythemia
Decreased conjugation
- Physiologic immaturity
- Prematurity
- Crigler–Najjar syndrome
- Gilbert syndrome
- Hypothyroidism
Increased enterohepatic circulation
- Breastfeeding jaundice (poor intake)
- Intestinal obstruction
Conjugated Hyperbilirubinemia (Cholestasis)
Always pathological:
- Biliary atresia
- Neonatal hepatitis
- TORCH infections
- Metabolic disorders (galactosemia)
5. Clinical Features
Mild jaundice
- Yellow skin starting from face → trunk → legs (Kramer rule)
Severe jaundice
- Lethargy
- Poor feeding
- Hypotonia
Signs of Acute Bilirubin Encephalopathy
- High-pitched cry
- Arching (opisthotonus)
- Seizures
- Apnea
Kernicterus (Chronic)
Permanent brain damage:
- Cerebral palsy
- Hearing loss
- Gaze abnormalities
6. Investigations / Diagnosis
Initial Tests
- Total serum bilirubin (TSB)
- Direct (conjugated) bilirubin
- Blood group of mother and baby
- Direct Coombs test
Hemolysis Workup
- CBC + reticulocyte count
- Peripheral smear
- G6PD screening
If prolonged jaundice (>14 days)
- LFTs
- Thyroid function tests
- Urine culture
- TORCH screen
7. Differential Diagnosis
- Physiologic jaundice
- Breastfeeding failure jaundice
- Breast milk jaundice
- Hemolytic disease
- Sepsis
- Hypothyroidism
- Biliary atresia (pale stools, dark urine)
8. Management (Stepwise)
A. General Measures
Feeding support
- Encourage breastfeeding 8–12 times/day
- Supplement if dehydration present
B. Phototherapy
Mechanism of Action
Phototherapy converts unconjugated bilirubin into water-soluble isomers:
- Lumirubin → excreted without conjugation
Indications
Based on bilirubin nomograms (AAP charts):
- Higher risk infants treated earlier:
* Prematurity
* Hemolysis
* Sepsis
Procedure
- Blue light wavelength: 430–490 nm
- Cover eyes + genitalia
- Monitor temperature and hydration
Adverse Effects
- Loose stools
- Dehydration
- Skin rash
- Bronze baby syndrome (cholestasis)
C. Exchange Transfusion
Used for life-threatening hyperbilirubinemia.
Indications
- Failure of intensive phototherapy
- Signs of bilirubin encephalopathy
- Very high bilirubin levels
Complications
- Electrolyte imbalance
- Infection
- Thrombocytopenia
- Catheter-related risks
D. IV Immunoglobulin (IVIG)
Used in immune hemolysis (Rh/ABO).
Drug Details (Required)
1. IVIG
- Indication: Hemolytic disease of newborn
- Mechanism: Blocks Fc receptors → reduces hemolysis
- Dose:
* 0.5–1 g/kg IV over 2 hours (may repeat)
- PK: Plasma proteins, half-life ~3 weeks
- Adverse Effects:
* Fever, hypotension
* Rare: anaphylaxis
- Contraindications:
* IgA deficiency with antibodies
- Monitoring:
* Bilirubin trend
* Hemolysis markers
- Counselling:
* Temporary infusion-related symptoms possible
2. Phenobarbital (Rare Use)
- Indication: Enhances bilirubin conjugation (rare)
- Mechanism: Induces UDP-glucuronyl transferase
- Dose:
* 3–5 mg/kg/day orally
- Adverse Effects:
* Sedation, respiratory depression
Not routine therapy.
9. Special Types of Jaundice
Breastfeeding Jaundice (Early)
- Day 2–5
- Due to poor intake
- Treat with feeding optimization
Breast Milk Jaundice (Late)
- After day 7
- Due to β-glucuronidase in milk
- Usually benign
Prolonged Jaundice
Always rule out:
- Biliary atresia (surgical emergency)
- Hypothyroidism
- Infection
10. Prevention
- Early and frequent feeding
- Bilirubin screening before discharge
- Follow-up within 48 hours for high-risk infants
11. Red Flags (Urgent Referral)
- Jaundice in first 24 hours
- Poor feeding, lethargy
- Pale stools, dark urine
- Rapid bilirubin rise
- Signs of encephalopathy
Summary Table
| Type | Onset | Cause | Risk |
| ------------- | -------- | ----------------- | --------- |
| Physiologic | >24h | Normal immaturity | Low |
| Hemolytic | <24h | ABO/Rh, G6PD | High |
| Breastfeeding | Day 2–5 | Poor intake | Moderate |
| Breast milk | Day 7–14 | Milk enzymes | Benign |
| Cholestasis | Any time | Biliary atresia | Dangerous |