Definition
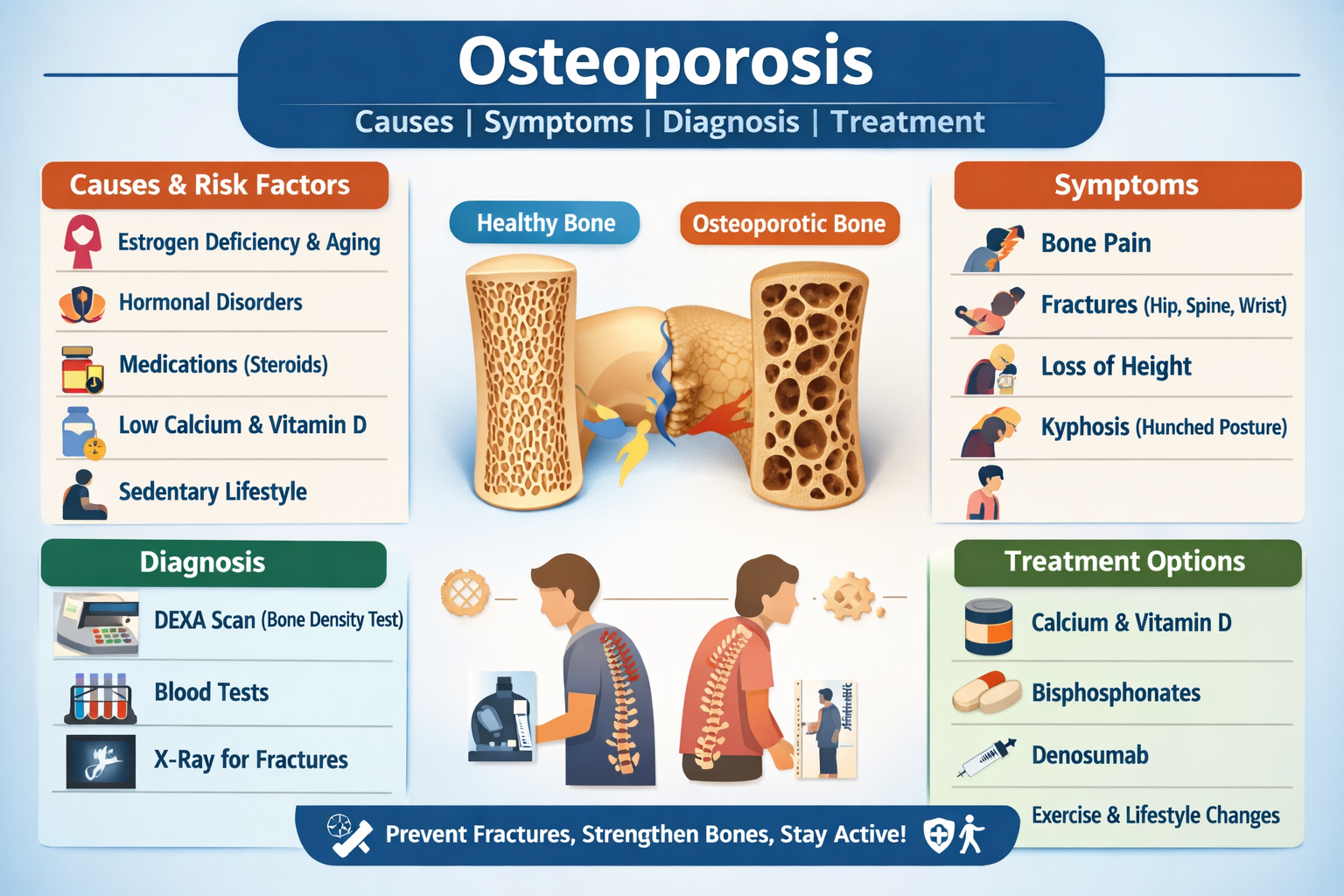
Osteoporosis is a chronic metabolic bone disease characterized by low bone mass, microarchitectural deterioration of bone tissue, and increased bone fragility, leading to a higher risk of fractures, especially in the hip, spine, and wrist.
Pathophysiology
- Bone remodeling normally balances bone formation (osteoblasts) and bone resorption (osteoclasts)
- In osteoporosis:
* Bone resorption exceeds bone formation
* Loss of bone density and structural strength occurs
- Estrogen deficiency, aging, hormonal imbalance, nutritional deficiencies, and inactivity accelerate bone loss
Causes and Risk Factors
Primary Osteoporosis
- Postmenopausal estrogen deficiency
- Age-related bone loss (senile osteoporosis)
- Genetic predisposition
Secondary Osteoporosis
- Endocrine disorders: Hyperthyroidism, Cushing syndrome, diabetes
- Chronic kidney or liver disease
- Rheumatoid arthritis
- Malabsorption syndromes (celiac disease)
- Cancer and chemotherapy
Medication-Induced
- Long-term corticosteroids
- Anticonvulsants
- Heparin
- Aromatase inhibitors
Lifestyle and Nutritional Causes
- Low calcium and vitamin D intake
- Smoking and alcohol abuse
- Sedentary lifestyle
- Low body weight
- Poor sunlight exposure
Clinical Features (Symptoms)
Early Stage
- Often asymptomatic (silent disease)
Progressive Symptoms
- Bone pain (especially back pain)
- Fragility fractures (fracture after minor trauma)
- Loss of height
- Kyphosis (stooped posture / dowager’s hump)
- Reduced mobility
Common Fracture Sites
- Hip
- Vertebrae (spine)
- Wrist (Colles fracture)
Complications
- Hip fractures leading to disability
- Chronic back pain
- Spinal deformity
- Reduced quality of life
- Increased mortality after major fractures
Investigations and Diagnosis
Bone Mineral Density (Gold Standard)
- DEXA scan
* T-score ≥ −1: Normal
* T-score −1 to −2.5: Osteopenia
* T-score ≤ −2.5: Osteoporosis
Laboratory Tests
- Serum calcium, phosphate
- Vitamin D levels
- Parathyroid hormone
- Thyroid function tests
- Renal and liver function tests
Imaging
- X-ray (vertebral fractures)
- MRI/CT if fracture suspected
Differential Diagnoses
- Osteomalacia
- Paget’s disease of bone
- Bone metastasis
- Rheumatoid arthritis
- Multiple myeloma
Management and Treatment (Comprehensive)
1. Lifestyle and Non-Pharmacologic Measures
- Weight-bearing exercises (walking, resistance training)
- Adequate sunlight exposure
- Smoking cessation
- Alcohol reduction
- Fall prevention strategies
- Balanced diet rich in calcium and protein
2. Calcium and Vitamin D Supplementation
Calcium
- Indication: Bone mineral support
- Dose: 1000–1200 mg/day (diet + supplements)
- Adverse Effects: Constipation, kidney stones
- Contraindications: Hypercalcemia
Vitamin D (Cholecalciferol)
- Dose: 800–2000 IU/day
- Role: Improves calcium absorption
- Monitoring: Serum vitamin D levels
3. Pharmacologic Treatment
A. Bisphosphonates (First-Line)
Examples: Alendronate, Risedronate, Zoledronic acid
- Mechanism: Inhibits osteoclast-mediated bone resorption
- Dose: Alendronate 70 mg once weekly
- Adverse Effects: GI irritation, osteonecrosis of jaw (rare)
- Contraindications: Esophageal disorders, severe renal impairment
B. Denosumab
- Mechanism: Monoclonal antibody inhibiting osteoclast activity
- Dose: 60 mg SC every 6 months
- Adverse Effects: Hypocalcemia, infection risk
- Indication: Postmenopausal osteoporosis, high fracture risk
C. Selective Estrogen Receptor Modulators (SERMs)
Example: Raloxifene
- Mechanism: Estrogen-like effect on bone
- Benefit: Reduces vertebral fractures
- Risk: Thromboembolism
D. Hormone Replacement Therapy (HRT)
- Used in postmenopausal women
- Benefits bone density
- Risks: Breast cancer, cardiovascular disease
E. Parathyroid Hormone Analogs
Example: Teriparatide
- Mechanism: Stimulates new bone formation
- Indication: Severe osteoporosis
- Duration: Max 2 years
F. Calcitonin
- Reduces bone resorption
- Provides pain relief in vertebral fractures
4. Fracture Management
- Surgical repair (hip fractures)
- Pain control
- Physical rehabilitation
- Fall prevention programs
Prevention Strategies
- Adequate calcium and vitamin D intake from early adulthood
- Regular physical activity
- Early screening after age 50 or high-risk individuals
- Minimizing long-term steroid use
Prognosis
- Early diagnosis and treatment reduce fracture risk
- Untreated osteoporosis leads to progressive disability
- Lifelong management improves bone strength and quality of life