1. Definition
Osteomyelitis is a serious bone infection caused by bacteria or fungi, leading to inflammation, bone destruction, necrosis, and sometimes chronic disability if untreated.
2. Pathophysiology (How Infection Develops)
Infection reaches bone through:
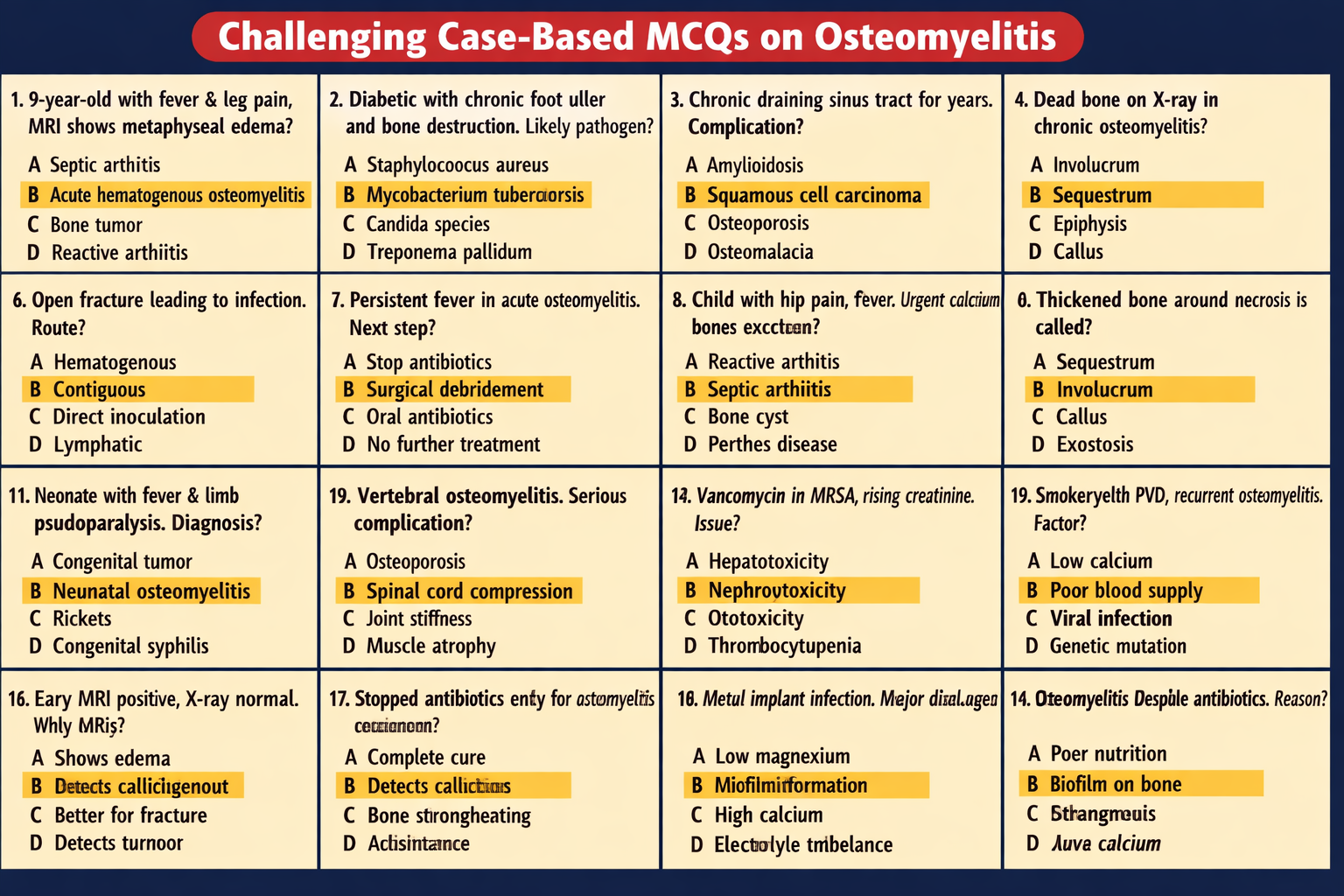
- Hematogenous spread (via bloodstream — common in children)
- Direct inoculation (open fractures, surgery, trauma)
- Contiguous spread (from nearby infected tissue, ulcers — common in diabetics)
Disease process:
- Pathogens invade bone marrow
- Inflammatory exudate increases pressure
- Reduced blood supply → bone necrosis
- Dead bone forms sequestrum
- New bone formation → involucrum
3. Causes and Common Pathogens
Bacterial Causes
- Staphylococcus aureus (most common)
- MRSA
- Streptococcus species
- Pseudomonas aeruginosa (IV drug users, trauma)
- Salmonella (sickle cell disease)
Fungal Causes
- Candida
- Aspergillus (immunocompromised)
4. Types of Osteomyelitis
A. Acute Osteomyelitis
- Rapid onset (days–weeks)
- Fever, severe pain, swelling
B. Chronic Osteomyelitis
- Persistent infection (>6 weeks)
- Sinus tracts, bone destruction, relapse risk
C. Hematogenous Osteomyelitis
- Spread via blood (children)
D. Post-Traumatic or Surgical Osteomyelitis
- After fractures or orthopedic surgery
E. Diabetic Foot Osteomyelitis
- Spread from chronic ulcers
5. Risk Factors
- Diabetes mellitus
- Trauma or surgery
- Immunosuppression
- IV drug use
- Poor circulation
- Chronic wounds
- Sickle cell disease
6. Clinical Features (Symptoms & Signs)
Local Symptoms
- Bone pain and tenderness
- Swelling, warmth, redness
- Restricted movement
- Sinus tract with pus (chronic)
Systemic Symptoms
- Fever, chills
- Fatigue
- Weight loss (chronic cases)
Pediatric Presentation
- Limping
- Refusal to bear weight
- Irritability
7. Investigations and Diagnosis
Laboratory Tests
- CBC → Elevated WBC
- ESR and CRP → Increased
- Blood culture → Identify organism
Imaging
- X-ray (late changes)
- MRI → Most sensitive (early detection)
- CT scan → Bone destruction
- Bone scan (if MRI unavailable)
Microbiological Confirmation
- Bone biopsy culture → Gold standard
8. Differential Diagnosis
- Bone tumors
- Septic arthritis
- Fractures
- Gout
- Tuberculous osteomyelitis
- Rheumatoid arthritis
9. Management (Stepwise Treatment)
A. Initial Management
- Hospital admission
- Pain control
- Immobilization
- Empirical IV antibiotics
B. Antibiotic Therapy (Core Treatment)
1. Vancomycin
- Indication: MRSA or resistant infections
- Mechanism: Inhibits bacterial cell wall synthesis
- Dose (Adult): 15–20 mg/kg IV every 8–12 hours
- Adverse Effects: Nephrotoxicity, Red man syndrome
- Contraindications: Severe renal impairment
- Monitoring: Kidney function, trough levels
- Counseling: Complete full course
2. Ceftriaxone
- Indication: Gram-negative and Streptococcus
- Mechanism: Cephalosporin inhibits cell wall synthesis
- Dose: 1–2 g IV once daily
- Adverse Effects: Allergy, GI upset
- Monitoring: Liver function
3. Clindamycin
- Indication: Staphylococcus, anaerobes
- Mechanism: Inhibits protein synthesis
- Dose: 600–900 mg IV every 8 hours
- Adverse Effects: C. difficile colitis
- Monitoring: Diarrhea symptoms
4. Linezolid
- Indication: Resistant Gram-positive bacteria
- Dose: 600 mg IV/PO every 12 hours
- Adverse Effects: Bone marrow suppression
- Monitoring: CBC weekly
5. Ciprofloxacin
- Indication: Gram-negative or Pseudomonas
- Dose: 400 mg IV every 12 hours
- Adverse Effects: Tendon rupture risk
- Avoid in: Children, pregnancy
Duration of Therapy
- Acute: 4–6 weeks
- Chronic: 6–12 weeks or longer
10. Surgical Management (If Needed)
Indications
- Abscess formation
- Dead bone (sequestrum)
- Failure of antibiotics
- Chronic infection
Procedures
- Debridement
- Drainage
- Removal of necrotic bone
- Bone grafting
- Amputation (severe cases)
11. Supportive and Non-Drug Care
- Rest and limb immobilization
- Nutritional support (high protein)
- Diabetes control
- Wound care
- Smoking cessation
- Physical rehabilitation after recovery
12. Complications
- Chronic infection
- Bone deformity
- Growth disturbance in children
- Septicemia
- Pathological fractures
- Amputation
- Malignancy in chronic sinus tracts (rare)
13. Prognosis
- Early treatment: Good outcome
- Delayed or chronic: High recurrence risk
- Diabetes and immunocompromised → Worse prognosis
14. Prevention
- Proper wound care
- Early treatment of infections
- Good diabetic foot care
- Sterile surgical practices
15. Patient Counseling Points
- Complete full antibiotic course
- Attend follow-up visits
- Monitor for fever, pain, swelling
- Maintain hygiene and wound care
- Avoid smoking
- Maintain nutrition and blood sugar control