Here is a concise but complete pediatric reference on Growth Hormone Deficiency (GHD) and Hypothyroidism (as per your requested structured format, no images):
1. Growth Hormone Deficiency (GHD) – Pediatrics
Definition
A disorder characterized by insufficient secretion of growth hormone (GH) from the anterior pituitary leading to impaired linear growth and short stature.
Pathophysiology
- GH → stimulates liver → IGF-1 (Somatomedin C) production
- IGF-1 → promotes epiphyseal growth (long bones)
- Deficiency → ↓ chondrocyte proliferation → reduced height velocity
- Also affects metabolism:
* ↓ lipolysis → ↑ fat
* ↓ protein synthesis → ↓ muscle mass
Causes / Triggers
Congenital
- Pituitary hypoplasia/aplasia
- Genetic mutations (GH1, GHRHR)
- Midline defects (cleft palate, septo-optic dysplasia)
Acquired
- Brain tumors (craniopharyngioma)
- CNS infections
- Trauma
- Irradiation
Idiopathic
- Most common
Clinical Features
Infants
- Hypoglycemia
- Prolonged jaundice
- Micropenis (boys)
Children
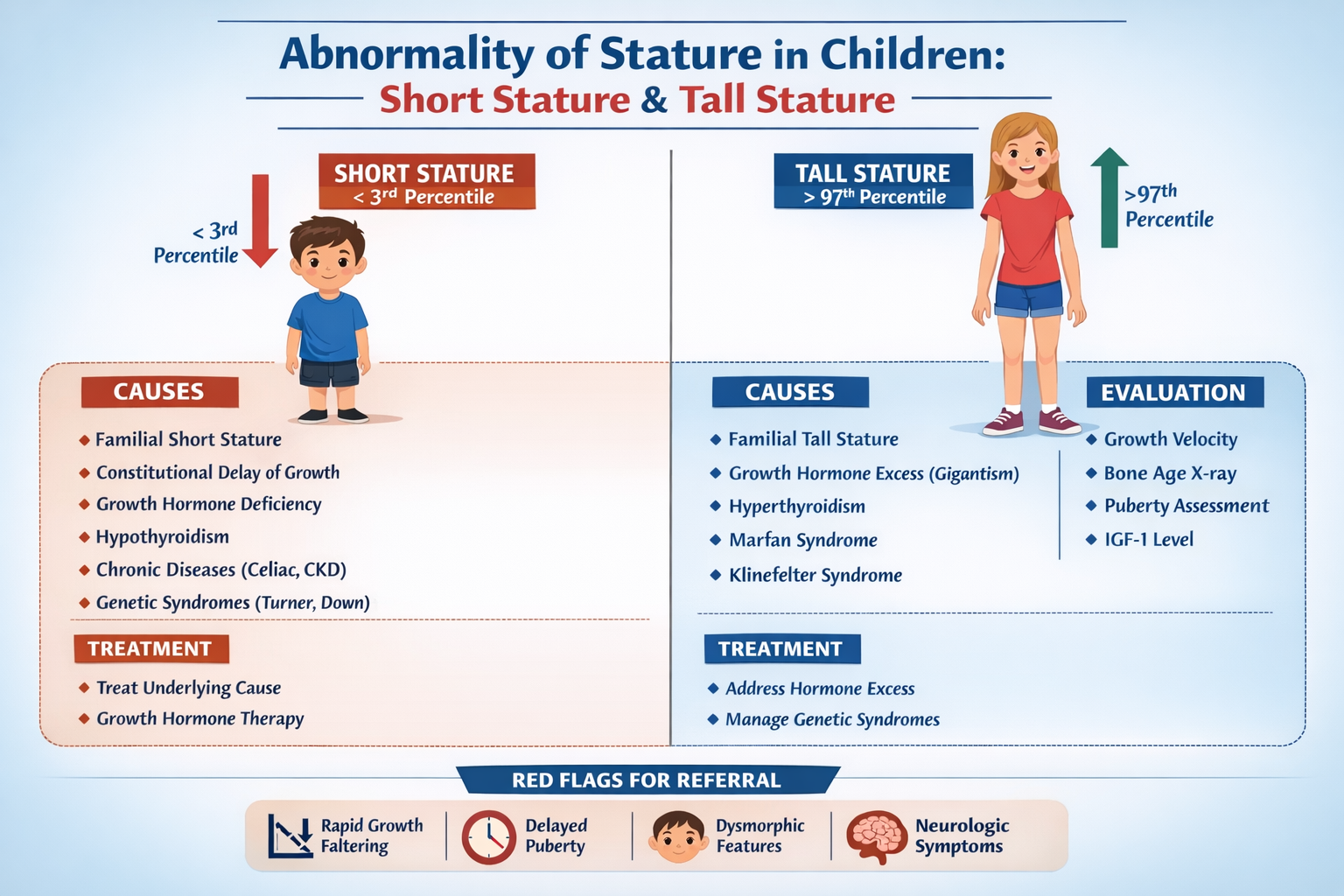
- Short stature (<3rd percentile)
- Decreased growth velocity
- Delayed bone age
- Increased fat (truncal obesity)
- Immature face (“doll-like”)
- Delayed puberty
Investigations / Diagnosis
- Growth chart: low height velocity
- Bone age X-ray (left wrist): delayed
- Serum IGF-1, IGFBP-3: low
- GH stimulation tests (gold standard)
* Insulin tolerance test
* Clonidine / arginine test
- MRI brain: pituitary abnormalities
Differential Diagnosis
- Familial short stature
- Constitutional delay
- Hypothyroidism
- Chronic systemic disease
- Turner syndrome
Management (Stepwise)
1. Recombinant GH therapy
Drug: Somatropin
- Indication: confirmed GHD
- Dose:
* 0.025–0.035 mg/kg/day SC (daily, evening)
- Mechanism: replaces GH → ↑ IGF-1 → bone growth
- PK: SC, short half-life, acts via IGF-1
- Adverse Effects
* Intracranial hypertension
* Slipped capital femoral epiphysis
* Edema, arthralgia
- Contraindications
* Active malignancy
- Monitoring
* Growth velocity
* IGF-1 levels
* Thyroid function
- Counselling
* Daily injections needed
* Early treatment → better outcomes
2. Treat underlying cause
- Tumor → surgery
- Hormone deficiencies → replace
Non-Pharmacological
- Nutrition optimization
- Psychosocial support
2. Hypothyroidism – Pediatrics
Definition
Deficiency of thyroid hormone (T3/T4) leading to impaired growth, neurodevelopment, and metabolism.
Pathophysiology
- Thyroid hormone regulates:
* Brain development
* Bone maturation
* Metabolism
- Deficiency →
* ↓ metabolic rate
* ↓ protein synthesis
* Irreversible intellectual disability (if untreated early)
Causes
Congenital Hypothyroidism
- Thyroid dysgenesis (agenesis, ectopia) – most common
- Dyshormonogenesis
- TSH receptor defects
Acquired Hypothyroidism
- Autoimmune (Hashimoto thyroiditis) – most common in older children
- Iodine deficiency
- Drugs (lithium, amiodarone)
- Post-thyroid surgery/radiation
Clinical Features
Neonates (often subtle early)
- Prolonged jaundice
- Constipation
- Poor feeding
- Hypotonia
- Large tongue (macroglossia)
- Umbilical hernia
Older children
- Short stature
- Weight gain
- Fatigue
- Cold intolerance
- Dry skin
- Delayed puberty
- Poor school performance
Investigations / Diagnosis
- TSH ↑, T4 ↓ (primary hypothyroidism)
- Newborn screening (TSH)
- Thyroid antibodies (anti-TPO)
- Thyroid scan (if needed)
- Bone age: delayed
Differential Diagnosis
- GHD
- Chronic illness
- Cushing syndrome
- Malnutrition
Management (Stepwise)
1. Thyroid Hormone Replacement
Drug: Levothyroxine
- Indication: all hypothyroid children
Dose
- Neonates: 10–15 mcg/kg/day
- Infants: 6–8 mcg/kg/day
- Children: 2–5 mcg/kg/day
Mechanism
- Synthetic T4 → converted to T3 → restores metabolism
Pharmacokinetics
- Oral absorption (best empty stomach)
- Long half-life (~7 days)
Adverse Effects
- Overdose → hyperthyroidism symptoms:
* Tachycardia
* Irritability
* Weight loss
Contraindications
- Untreated adrenal insufficiency (relative)
Drug Interactions
- Iron, calcium ↓ absorption
- Antiepileptics ↑ metabolism
Monitoring
- TSH, T4 every:
* 2–4 weeks (initial)
* Then every 3–6 months
Counselling
- Give on empty stomach
- Lifelong therapy (most cases)
- Early treatment prevents intellectual disability
2. Early treatment in neonates
- Start within first 2 weeks of life
- Prevents cretinism (severe neurodevelopmental delay)
Non-Pharmacological
- Adequate iodine intake
- Growth and development monitoring
Key Comparison (Exam Quick Table)
| Feature | GHD | Hypothyroidism |
| --------------- | ------------- | -------------- |
| Growth velocity | ↓↓↓ | ↓ |
| Weight | Normal/↑ fat | ↑ |
| Bone age | Delayed | Delayed |
| IQ | Normal | ↓ if untreated |
| Hormone defect | GH | T3/T4 |
| Treatment | GH injections | Levothyroxine |
If you want, I can also provide MCQs, case-based questions, or quick revision notes for exam prep.