Respiratory Distress in Newborn (Neonatal Respiratory Distress)
Definition
Respiratory distress in a newborn refers to difficulty in breathing occurring soon after birth or within the first few days of life. It is a common neonatal emergency requiring rapid evaluation.
Clinical Features (Signs of Respiratory Distress)
Newborns show distress when they cannot maintain normal oxygenation.
Key Signs
- Tachypnea: Respiratory rate > 60/min
- Nasal flaring
- Chest retractions
* Subcostal
* Intercostal
* Suprasternal
- Grunting
- Cyanosis
* Central cyanosis indicates hypoxemia
- Apnea episodes
- Poor feeding
- Lethargy or irritability
Pathophysiology
Respiratory distress results from:
- Inadequate lung expansion
- Impaired gas exchange
- Airway obstruction
- Pulmonary hypertension
- Infection or inflammation
- Structural abnormalities
Causes of Respiratory Distress in Newborn (Detailed Classification)
Respiratory distress has many causes, broadly divided into:
1. Respiratory (Pulmonary) Causes
A. Respiratory Distress Syndrome (RDS / Hyaline Membrane Disease)
Most common in premature infants
Cause
- Surfactant deficiency → alveolar collapse
Risk Factors
- Prematurity (<34 weeks)
- Maternal diabetes
- Cesarean delivery without labor
Features
- Onset within minutes–hours after birth
- Progressive worsening distress
- Ground-glass appearance on X-ray
B. Transient Tachypnea of the Newborn (TTN)
Delayed clearance of fetal lung fluid
Risk Factors
- Term or late-preterm babies
- Cesarean section
- Maternal asthma
Features
- Mild–moderate tachypnea
- Improves within 24–72 hours
C. Meconium Aspiration Syndrome (MAS)
Seen in post-term or stressed babies
Mechanism
- Meconium inhaled → airway obstruction + chemical pneumonitis
Features
- Respiratory distress at birth
- Green-stained liquor
- Patchy infiltrates on X-ray
Complications:
- Persistent pulmonary hypertension (PPHN)
- Air leaks
D. Pneumonia (Congenital or Early-Onset)
Infection acquired before or during delivery
Common Organisms
- Group B Streptococcus
- E. coli
- Listeria
Features
- Respiratory distress + sepsis signs
- Poor feeding, temperature instability
E. Pneumothorax (Air Leak Syndrome)
Air escapes into pleural space → lung collapse
Causes
- Mechanical ventilation
- MAS
- RDS
Signs
- Sudden deterioration
- Asymmetric chest movement
- Decreased breath sounds
F. Pulmonary Hemorrhage
Seen in
- Prematurity
- Severe RDS
- PDA
Signs
- Bloody secretions
- Sudden hypoxia
G. Bronchopulmonary Dysplasia (BPD)
Chronic lung disease of prematurity
Cause
- Prolonged oxygen therapy/ventilation
2. Cardiovascular Causes
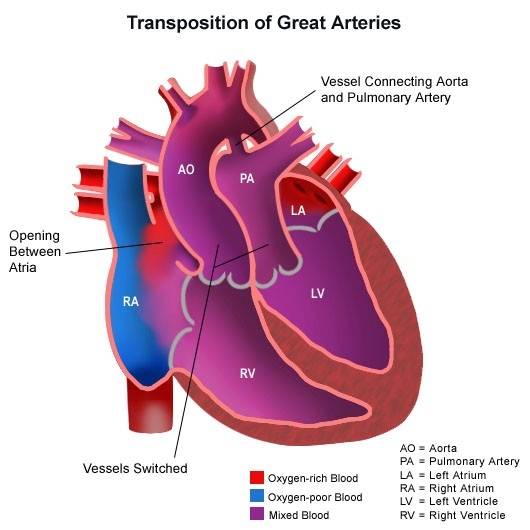
A. Congenital Heart Disease (CHD)
Certain CHDs present with respiratory distress:
- Transposition of great arteries
- Tetralogy of Fallot
- Total anomalous pulmonary venous return (TAPVR)
Clues
- Cyanosis not improving with oxygen
- Murmurs
- Poor perfusion
B. Persistent Pulmonary Hypertension of Newborn (PPHN)
Failure of normal drop in pulmonary vascular resistance after birth.
Causes
- MAS
- Sepsis
- Asphyxia
Features
- Severe hypoxemia
- Pre-ductal vs post-ductal saturation difference
C. Heart Failure
Due to structural defects or myocarditis.
Signs:
- Tachypnea
- Hepatomegaly
- Poor feeding
3. Infectious Causes
A. Neonatal Sepsis
Systemic infection → respiratory distress
Signs
- Poor feeding
- Temperature instability
- Apnea
- Shock
Organisms:
- GBS
- E. coli
- Klebsiella
B. Viral Infections
- RSV
- CMV
- Influenza
4. Airway Obstruction Causes
A. Choanal Atresia
Blocked posterior nasal passages
Features
- Cyanosis improves when crying
- Difficulty feeding
B. Pierre Robin Sequence
- Micrognathia
- Glossoptosis
- Cleft palate
Airway obstruction especially when supine.
C. Laryngeal Web / Tracheomalacia
- Stridor
- Noisy breathing
D. Congenital Diaphragmatic Hernia (CDH)
Abdominal organs herniate into chest.
Features
- Severe distress at birth
- Scaphoid abdomen
- Mediastinal shift
5. Neurologic Causes
A. Birth Asphyxia / Hypoxic-Ischemic Encephalopathy
Depressed respiratory drive
Signs:
- Poor tone
- Weak cry
- Apnea
B. Intracranial Hemorrhage
Seen in preterm infants.
C. Maternal Drug Exposure
Sedatives/opioids → respiratory depression.
6. Metabolic Causes
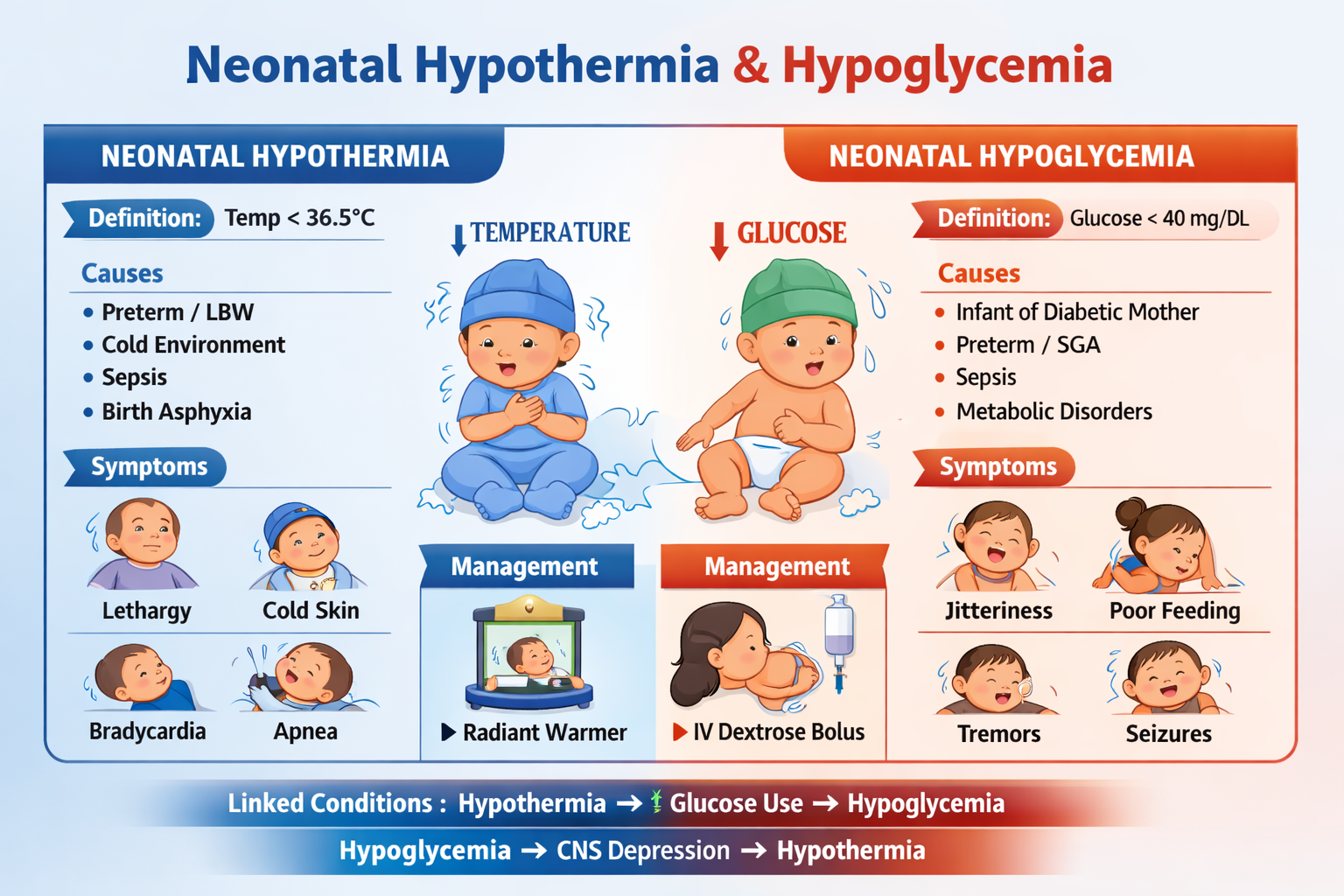
A. Hypoglycemia
Can cause apnea and distress.
B. Hypocalcemia
Leads to jitteriness, seizures, poor breathing.
C. Inborn Errors of Metabolism
Acidosis → compensatory tachypnea.
7. Hematologic Causes
A. Anemia
Reduced oxygen delivery → tachypnea.
B. Polycythemia
Hyperviscosity → poor perfusion, distress.
8. Miscellaneous Causes
A. Temperature Instability
Cold stress increases oxygen consumption → distress.
B. Gastroesophageal Reflux / Aspiration
Milk aspiration causes tachypnea and cough.
Approach to Diagnosis
History
- Gestational age
- Mode of delivery
- Meconium staining
- Maternal fever/infection
Examination
- Respiratory rate
- Retractions, cyanosis
- Heart murmur
- Perfusion
Investigations
- Pulse oximetry
- Chest X-ray
- ABG
- Blood culture
- CBC, CRP
- Echocardiography if CHD suspected
Management Principles (General)
- Maintain airway and breathing
- Oxygen therapy
- CPAP or ventilation if needed
- Treat underlying cause:
* Surfactant for RDS
* Antibiotics for infection
* Chest tube for pneumothorax
* Surgery for diaphragmatic hernia
Summary Table (Quick View)
| Cause | Typical Baby | Onset |
| ---------------- | ------------------------- | -------------------- |
| RDS | Preterm | Immediate |
| TTN | Term, C-section | Early, resolves fast |
| MAS | Post-term, fetal distress | At birth |
| Pneumonia/Sepsis | Any | Within 24–72h |
| Pneumothorax | Ventilated/MAS | Sudden |
| CHD/PPHN | Term | Severe cyanosis |