Below is a concise but complete pediatric reference for both conditions, following the structured format you prefer.
Neonatal Hypothermia
Definition
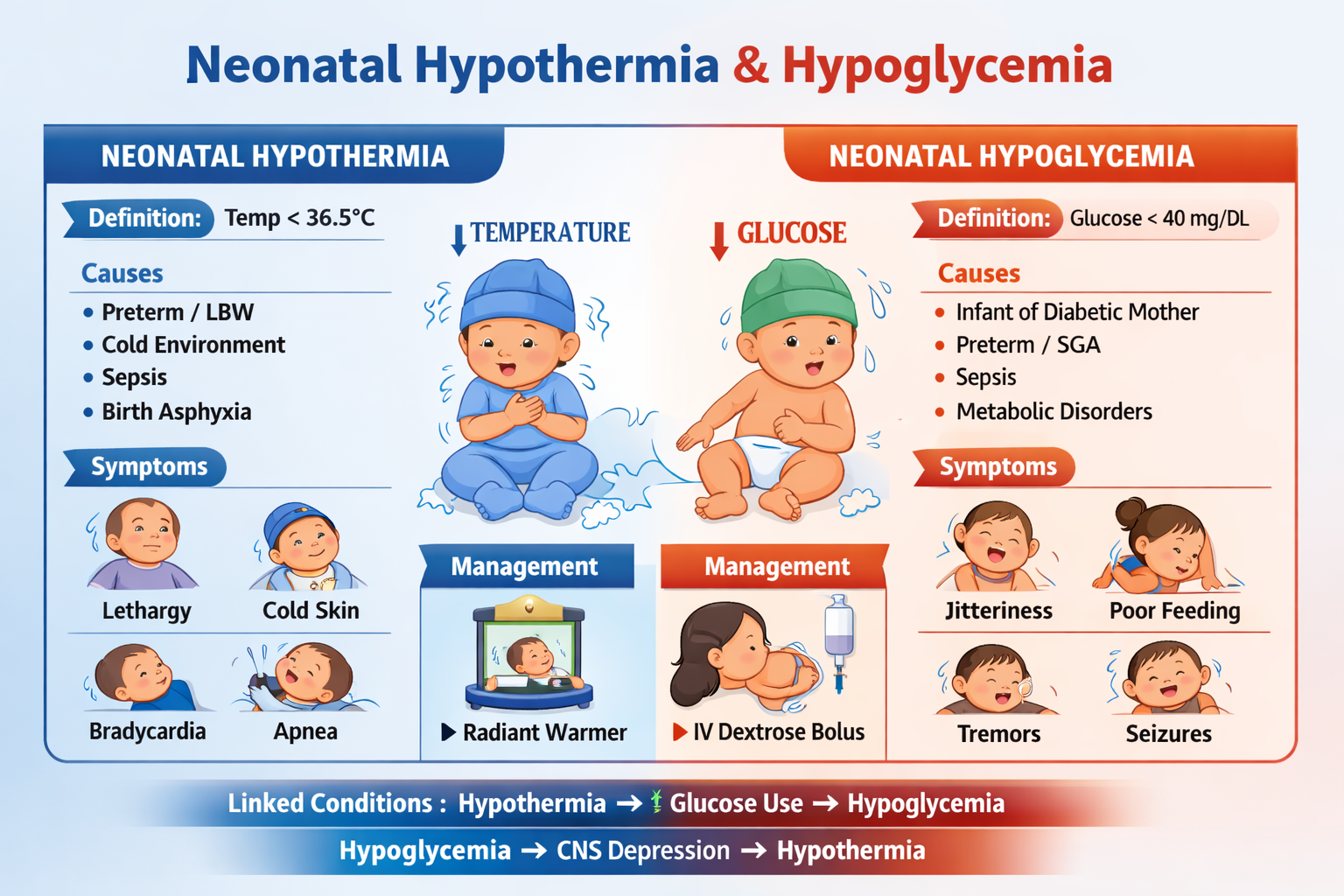
Neonatal hypothermia is a condition in which the core body temperature of a newborn falls below 36.5°C (97.7°F).
According to the World Health Organization classification:
| Severity | Temperature |
| ------------------ | ----------- |
| Mild (Cold stress) | 36.0–36.4°C |
| Moderate | 32.0–35.9°C |
| Severe | <32°C |
Pathophysiology
Newborns are prone to hypothermia due to:
- Large surface area to body mass ratio
- Thin skin with minimal subcutaneous fat
- Immature thermoregulation
- Limited shivering mechanism
Heat loss occurs through four mechanisms:
- Evaporation – loss from wet skin after birth
- Conduction – contact with cold surfaces
- Convection – heat lost to surrounding air
- Radiation – transfer to colder nearby objects
To generate heat, neonates rely on non-shivering thermogenesis via brown adipose tissue.
Cold stress increases:
- Oxygen consumption
- Glucose utilization
- Anaerobic metabolism
- Risk of metabolic acidosis and hypoglycemia
Causes / Risk Factors
Environmental
- Low delivery room temperature
- Delayed drying after birth
- Inadequate clothing or warming
Neonatal Factors
- Prematurity
- Low birth weight
- Birth asphyxia
- Sepsis
- Hypoglycemia
Maternal Factors
- Prolonged labor
- Cesarean section without warming
- Maternal sedation
Clinical Features
Early Signs
- Cold extremities
- Lethargy
- Poor feeding
- Weak cry
Progressive Signs
- Hypotonia
- Bradycardia
- Apnea
- Cyanosis
- Metabolic acidosis
- Hypoglycemia
Severe Complications
- Respiratory distress
- Coagulopathy
- Shock
- Death
Investigations / Diagnosis
Clinical Diagnosis
- Measure axillary temperature
Laboratory Tests
- Blood glucose
- Blood gas analysis
- Serum electrolytes
- Sepsis screen if infection suspected
Differential Diagnosis
- Neonatal Sepsis
- Hypoglycemia
- Birth Asphyxia
- Respiratory Distress Syndrome
Management
Immediate Management
Mild Hypothermia (36–36.4°C)
- Skin-to-skin contact (kangaroo care)
- Warm clothing
- Cap and socks
- Early breastfeeding
- Monitor temperature every 30 min
Moderate Hypothermia (32–35.9°C)
- Use radiant warmer or incubator
- Warm blankets
- Monitor temperature every 15–30 min
- Check blood glucose
- Treat hypoglycemia if present
Severe Hypothermia (<32°C)
- Intensive warming under radiant warmer
- Warmed IV fluids
- Oxygen therapy
- Cardiorespiratory monitoring
- Treat complications
Non-Pharmacologic Prevention
- Warm delivery room (≥25°C)
- Immediate drying
- Delayed bathing
- Early breastfeeding
- Kangaroo mother care
- Use of caps and warm clothing
Neonatal Hypoglycemia
Definition
Neonatal hypoglycemia is defined as low plasma glucose concentration in a newborn.
Common clinical thresholds:
| Age | Hypoglycemia |
| -------------- | ------------ |
| First 4 hours | <40 mg/dL |
| 4–24 hours | <45 mg/dL |
| After 24 hours | <50 mg/dL |
Pathophysiology
During fetal life:
- Glucose supplied by placenta.
After birth:
- Placental supply stops.
- Neonate depends on:
* Glycogenolysis
* Gluconeogenesis
* Fat metabolism
Hypoglycemia occurs when:
- Glucose production < glucose utilization
Major mechanisms:
- Hyperinsulinism
- Depleted glycogen stores
- Increased metabolic demand
Causes
Maternal Causes
- Diabetes mellitus
- Maternal medications (beta blockers)
Neonatal Causes
- Prematurity
- Small for gestational age
- Large for gestational age
- Birth asphyxia
- Sepsis
- Hypothermia
Metabolic Disorders
- Hyperinsulinism
- Inborn errors of metabolism
- Hormonal deficiency
Clinical Features
Often Asymptomatic
Symptomatic Features
- Jitteriness
- Tremors
- Poor feeding
- Lethargy
- Hypotonia
- Apnea
- Seizures
- Cyanosis
Severe untreated hypoglycemia can lead to brain injury.
Investigations
Bedside Tests
- Capillary blood glucose
Laboratory Tests
- Plasma glucose
- Serum insulin
- Cortisol
- Growth hormone
- Blood gas
- Sepsis screen
Differential Diagnosis
- Neonatal Sepsis
- Hypocalcemia
- Birth Asphyxia
- Intracranial Hemorrhage
Management
Asymptomatic Hypoglycemia
- Early breastfeeding
- Oral glucose gel
- Repeat glucose monitoring
Symptomatic Hypoglycemia
Drug Therapy
1. Dextrose
Indication
Treatment of neonatal hypoglycemia.
Mechanism of Action
Provides immediate glucose for cellular metabolism.
Dose
Initial bolus:
- 2 mL/kg of 10% dextrose IV
Continuous infusion:
- 6–8 mg/kg/min glucose infusion rate
Pharmacokinetics
- Rapid distribution
- Immediate metabolic use
Common Adverse Effects
- Hyperglycemia
- Fluid overload
Serious Adverse Effects
- Electrolyte imbalance
Contraindications
- Severe hyperglycemia
Drug Interactions
Minimal significant interactions.
Monitoring
- Blood glucose every 30–60 min initially
Patient Counseling (Parents)
- Importance of early feeding
- Monitoring signs like jitteriness or poor feeding
Non-Pharmacologic Measures
- Early breastfeeding within 1 hour of birth
- Maintain body temperature
- Frequent feeds
- Kangaroo mother care
Complications
Untreated hypoglycemia may lead to:
- Seizures
- Developmental delay
- Cerebral palsy
- Brain injury
If you want, I can also give exam-focused points for pediatric viva and MCQ (very high yield for NEET-PG / NEXT / USMLE) for these two neonatal conditions.